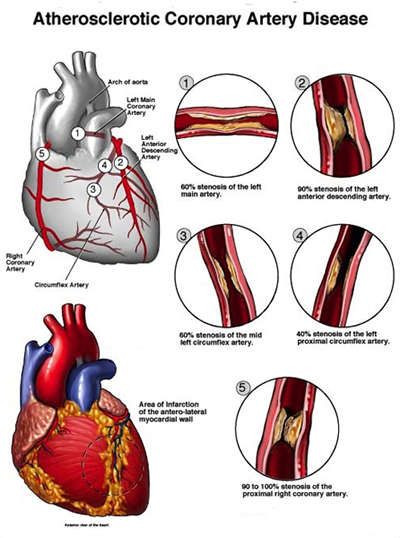
Part II Causes of CAD:
Coronary artery disease is thought to begin with damage or injury to the inner layer of a coronary artery, sometimes as early as childhood. The damage may be caused by various factors, including the following which are problems we can prevent or better control through better diet, some form of exercise balanced with rest. Including keeping our stress controlled in a productive way (like work out program to doing hobbies).
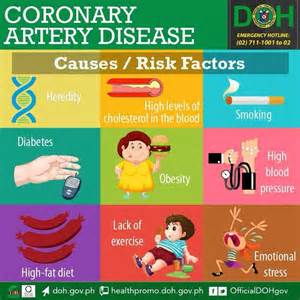
Causes that are modifiable (that we can change or help control):
- Smoking-Stop it
- High blood pressure-Lose weight, decrease junk food and sodium in your diet, exercise. If on B/P meds be compliant in taking them.
- High cholesterol-Eat better food, lose weight, or if on anti-cholesterol meds be compliant in taking them.
- Diabetes or insulin resistance-Lose weight, eat foods=no sugar, and be compliant with your diabetic meds.
- Sedentary lifestyle-Get in an exercise program; stay active.
Causes that are nonmodifiable (that you can’t change):
-Race: Race refers to common characteristics passed down through the genes. Non-Hispanic whites (63%) have roots in Europe, the Middle East, or North Africa. Blacks (13%) have origins in any of the black racial groups of Africa or Afro-Caribbean countries. Asians (5%) may have ancestors anywhere from India to Japan. This geographic diversity within racial groups means that there are actually greater genetic differences within than between certain groups.
Know this: Rates of high blood pressure, diabetes, and heart disease vary among people of different backgrounds.
Adults living in the United States are more likely to die from heart disease than any other cause, regardless of their racial or ethnic heritage. But certain minority groups face a greater risk than others. These differences appear to stem from an increased prevalence of high blood pressure, diabetes, and obesity seen in some populations compared with white Americans.
Still, teasing out the reasons isn’t easy. Genetic differences do exist. But diversity within different racial and ethnic groups means that genetic traits common to some groups can’t be generalized to an entire race.
Many intertwined factors likely contribute to the higher heart disease rates seen among some groups. Their lower average incomes affect where they live, which in turn affects their access to healthy food, safe places to exercise, and quality health care. In other words, “your ZIP code is more important than your genetic code,” says Dr. Eldrin Lewis, a cardiologist at Harvard-affiliated Brigham and Women’s Hospital.
But even after adjustment for factors related to socioeconomic differences, disparities in rates of heart disease and its risk factors persist, Dr. Lewis says. In the United States, nearly half of all black adults have some form of cardiovascular disease, compared with about one-third of all white adults. A genetic difference that predisposes blacks to high blood pressure might play a role.
For further details on race groups and their risk at coronary heart disease see https://www.health.harvard.edu/heart-health/race-and-ethnicity
–Heredity: A family history of heart disease is associated with a higher risk of coronary artery disease, especially if a close relative developed heart disease at an early age. Your risk is highest if your father or a brother was diagnosed with heart disease before age 55 or if your mother or a sister developed it before age 65.
-Age:Just like a car the older you get the highier the risk of problems with the vehicle and the same with the body.
-Gender: Men are generally at greater risk of coronary artery disease. However, the risk for women increases after menopause.
Learn more tomorrow on treatment of CAD in Part III!