“All children may experience very stressful events that affect how they think and feel. Most of the time, children recover quickly and well. However, sometimes children who experience severe stress, such as from an injury, from the death or threatened death of a close family member or friend, or from violence, will be affected long-term. The first step to treatment is to talk with a healthcare provider to arrange an evaluation. For a PTSD diagnosis, a specific event must have triggered the symptoms. Once the diagnosis is made, the first step is to make the child feel safe by getting support from parents, friends, and school, and by minimizing the chance of another traumatic event to the extent possible. Psychotherapy in which the child can speak, draw, play, or write about the stressful. Behavior therapy, specifically cognitive-behavioral therapy, helps children learn to change thoughts and feelings by first changing behavior in order to reduce the fear or worry. Medication may also be used to. Even though PTSD treatments work, most people who have PTSD don’t get the help they need. June is PTSD Awareness Month. Help spread the word that effective PTSD treatments are available.“.
Centers for Disease Control and Prevention – CDC (https://www.cdc.gov)
“Posttraumatic stress disorder (PTSD) is a mental health problem. PTSD can only develop after you go through or see a life-threatening event. It’s normal to have stress reactions to these types of events, and most people start to feel better after a few weeks or months. Learn about PTSD symptoms and treatments to help you get better. There are currently about 8 million people in the United States with PTSD.”.
U.S. Dept of Veterans Affairs (https://www.ptsd.va.gov)
“Alice in Wonderland syndrome (AIWS) is a rare neurological disorder characterized by distortions of visual perception (metamorphopsias), the body image, and the experience of time, along with derealization and depersonalization. Some 85% of patients present with perceptual distortions in a single sensory modality, e.g., only visual or only somesthetic in nature. Moreover, the majority experience only a single type of distortion, e.g., only micropsia or only macropsia. AIWS has many different etiologies, and hence an extensive differential diagnosis. Its amenability to treatment depends on the underlying pathological process, which in children is mostly encephalitis, and in adults, migraine.”.
Frontiers in Neurology (https://www.frontiersin.org).
While there currently is no identified genetic locus/loci associated with Alice in Wonderland Syndrome, observations suggest that a genetic component does exist. AiWS does appear to be passed on from parent to child, with one case study showcasing a grandmother, mother, son, and daughter all with Alice in Wonderland Syndrome. In addition, there is an established hereditary trait of migraines. Examples of environmental influences on the incidence of AiWS include the use of the drug topiramate and potentially the dietary intake of tyramine. Further research is required to establish the genetic and environmental influences on Alice in Wonderland Syndrome.
Alice in Wonderland
Alice in Wonderland Syndrome was named after Lewis Carroll’s famous 19th-century novel Alice’s Adventures in Wonderland. In the story, Alice, the title character, experiences numerous situations similar to those of micropsia and macropsia. The thorough descriptions of metamorphosis clearly described in the novel were the first of their kind to depict the bodily distortions associated with the condition. Speculation has arisen that Carroll may have written the story using his own direct experience with episodes of micropsia resulting from the numerous migraines he was known to suffer from. It has also been suggested that Carroll may have suffered from temporal lobe epilepsy.
Gulliver’s Travels
Alice in Wonderland Syndrome’s symptom of micropsia has also been related to Jonathan Swift’s novel Gulliver’s Travels. It has been referred to as “Lilliput sight” and “Lilliputian hallucination”, a term coined by British physician Raoul Leroy in 1909, based on the small people that inhabited the island of Lilliput in the novel.
Etiology
Complete and partial forms of the Alice in Wonderland syndrome exist in a range of disorders, including epilepsy, intoxicants, infectious states, fevers, and brain lesions. Furthermore, the syndrome is commonly associated with migraines, as well as the use of psychoactive drugs. It can also be the initial symptom of the Epstein–Barr virus (see mononucleosis), and a relationship between the syndrome and mononucleosis has been suggested. Epstein-Barr Virus appears to be the most common cause in children, while for adults it is more commonly associated with migraines.
Cerebral hypotheses
AiWS can be caused by abnormal amounts of electrical activity causing abnormal blood flow in the parts of the brain that process visual perception and texture. Nuclear medical techniques using technetium, performed on patients during episodes of Alice in Wonderland syndrome, have demonstrated that AiWS is associated with reduced cerebral perfusion in various cortical regions (frontal, parietal, temporal and occipital), both in combination and in isolation. It has been hypothesized that any condition resulting in a decrease in perfusion of the visual pathways or visual control centers of the brain may be responsible for the syndrome. For example, one study used single photon emission computed tomography to demonstrate reduced cerebral perfusion in the temporal lobe in patients with AiWS. Other theories exist that suggest the syndrome is a result of unspecific cortical dysfunction (e.g. from encephalitis, epilepsy, decreased cerebral perfusion), or reduced blood flow to other areas of the brain. Other theories suggest that disordered body image perceptions stem from within the parietal lobe. This has been demonstrated by the production of disturbances of body image through electrical stimulation of the posterior parietal cortex. Other researchers suggest that metamorphopsias may be a result of reduced perfusion of the non-dominant posterior parietal lobe during migraine episodes.
Throughout all the neuroimaging studies, several cortical regions (including the temporoparietal junction within the parietal lobe, and the visual pathway, specifically the occipital lobe) are associated with the development of Alice in Wonderland syndrome symptoms.
Migraines
The role of migraines in Alice in Wonderland syndrome is still not understood, but both vascular and electrical theories have been suggested. For example, visual distortions may be a result of transient, localized ischaemia (an inadequate blood supply to an organ or part of the body) in areas of the visual pathway during migraine attacks. In addition, a spreading wave of depolarization of cells (particularly glial cells) in the cerebral cortex during migraine attacks can eventually activate the trigeminal nerve’s regulation of the vascular system. The intense cranial pain during migraines is due to the connection of the trigeminal nerve with the thalamus and thalamic projections onto the sensory cortex. Alice in Wonderland syndrome symptoms can precede, accompany, or replace the typical migraine symptoms.
Diagnosis
Alice in Wonderland syndrome is a disturbance of perception rather than a specific physiological change to the body’s systems. The diagnosis can be presumed when other causes have been ruled out and if the patient presents symptoms along with migraines and complains of onset during the day (although it can also occur at night). As there are no established diagnostic criteria for Alice in Wonderland syndrome, there is likely to be a large degree of variability in the diagnostic process and thus it is likely to be poorly diagnosed.
Prognosis
Whatever the cause, the bodily related distortions can recur several times a day and may take some time to abate. Understandably, the person can become alarmed, frightened, and panic-stricken throughout the course of the hallucinations—maybe even hurt themselves or others around them. The symptoms of the syndrome themselves are not harmful and are likely to disappear with time. The outcome is typically not harmful, especially in children, and most patients outgrow these episodes. The long-term prognosis typically depends on the root cause of the syndrome, and it is the underlying condition which must be evaluated and treated. Often, the difficulty lies within the patient’s reluctance to describe their symptoms out of fear of being labeled with a psychiatric disorder.
Treatment
At present, Alice in Wonderland syndrome has no standardized treatment plan. Often, treatment methods revolve around migraine prophylaxis, as well as the promotion of a low tyramine diet. Drugs that may be used to prevent migraines include: anticonvulsants, antidepressants, calcium channel blockers, and beta blockers. Other treatments that have been explored include repetitive transcranial magnetic stimulation (rTMS). Further research is required to establish an effective treatment regime.
Epidemiology
The lack of established diagnostic criteria or large-scale epidemiological studies on Alice in Wonderland syndrome means that the exact prevalence of the syndrome is currently unknown. One study on 3,224 adolescents in Japan demonstrated the occurrence of macropsia and micropsia to be 6.5% in boys and 7.3% in girls, suggesting that the symptoms of AiWS may not be so rare.
It appears that the male/female ratio is dependent on the age range being observed. Studies showed that younger males (age range of 5 to 14 years) were 2.69 times more likely to experience AiWS than girls of the same age, while there were no significant differences between students of 13 to 15 years of age. Conversely, female students (16- to 18-year-olds) showed a significantly greater prevalence.
The average age of the start of Alice in Wonderland syndrome is six but it is very normal for some to experience the syndrome from childhood to their late 20’s. It is also thought that this syndrome is hereditary because many parents who have AiWS report their children having it as well.
Alice in Wonderland Syndrome (AiWS), also known as Todd’s syndrome or dysmetropsia, is a disorienting neuropsychological condition that affects perception. People may experience distortions in visual perception such as micropsia (objects appearing small), macropsia (objects appearing large), pelopsia (objects appearing to be closer than they are), or teleopsia (objects appearing to be further away than they are). Size distortion may occur in other sensory modalities as well.
The syndrome is sometimes called Todd’s syndrome, in reference to an influential description of the condition in 1955 by Dr. John Todd (1914-1987), a British Consultant Psychiatrist at High Royds Hospital at Menston in West Yorkshire. Todd discovered that several of his patients experienced severe headaches causing them to see and perceive objects as greatly out of proportion. They have altered sense of time and touch, as well as distorted perceptions of their own body. Although having migraine headaches, none of these patients had brain tumors, damaged eyesight, or mental illness that could have caused similar symptoms. They were also all able to think lucidly and could distinguish hallucinations from reality, however, their perceptions were skewed.
Since Lewis Carroll had been a well-known migraine sufferer with similar symptoms, Todd speculated that Carroll had used his own migraine experiences as a source of inspiration for his famous 1865 novel Alice’s Adventures in Wonderland. Carroll’s diary reveals that in 1856 he consulted William Bowman, an eminent ophthalmologist, about the visual manifestations of the migraines he regularly experienced. Since Carroll had these migraine symptoms for years before writing Alice’s Adventures, it seemed reasonable that Carroll had used his experiences as inspiration.
AiWS is often associated with migraines, brain tumors, and psychoactive drug use. It can also be the initial symptom of the Epstein–Barr Virus (see mononucleosis). AiWS can be caused by abnormal amounts of electrical activity resulting in abnormal blood flow in the parts of the brain that process visual perception and texture.
Anecdotal reports suggest that the symptoms are common in childhood, with many people growing out of it in their teen years. It appears that AiWS is also a common experience at sleep onset and has been known to commonly arise due to a lack of sleep.
Signs and symptoms
AiWS is often associated with migraines. AiWS affects the sense of vision, sensation, touch, and hearing, as well as one’s own body image.Nausea, dizziness, and agitation are also commonly associated symptoms with Alice in Wonderland Syndrome.
Individuals with AiWS can experience hallucinations or illusions of expansion, reduction or distortion of their own body image, such as microsomatognosia (feeling that their own body or body parts are shrinking), or macrosomatognosia (feeling that their body or body parts are growing taller or larger). These changes in perception are collectively known as metamorphosias, or Lilliputian hallucinations.
People with certain neurological diseases have experienced similar visual hallucinations. These hallucinations are called “Lilliputian”, which means that objects appear either smaller or larger than reality.
Patients may experience either micropsia or macropsia. Micropsia is an abnormal visual condition, usually occurring in the context of visual hallucination, in which the affected person sees objects as being smaller than they are in reality. Macropsia is a condition where the individual sees everything larger than it actually is.
One 17-year-old man described his odd symptoms by the following: “Quite suddenly objects appear small and distant or large and close. I feel as [if] I am getting shorter and smaller ‘shrinking’ and also the size of persons are not longer than my index finger (a lilliputian proportion). Sometimes I see the blind in the window or the television getting up and down, or my leg or arm is swinging. I may hear the voices of people quite loud and close or faint and far. Occasionally, I experience attacks of migrainous headache associated with eye redness, flashes of lights and a feeling of giddiness. I am always conscious to the intangible changes in myself and my environment”.
Although a person’s eyes are normal, they will often ‘see’ objects as the incorrect size, shape or perspective angle. Therefore, people, cars, buildings, houses, animals, trees, environments, etc., look smaller or larger than they should be. Further, depth perception can be altered whereby perceived distances are incorrect. For example, a corridor may appear to be very long, or the ground may appear too close.
Zoopsias is an additional hallucination that is sometimes associated with Alice in Wonderland Syndrome. Zoopsias involves hallucinations of either swarms of small animals (e.g. ants and mice etc.), or isolated groups of larger animals (e.g. dogs and elephants etc.). This experience of zoopsias is shared in a variety of conditions, such as delirium tremens.
The person affected by Alice in Wonderland syndrome may also lose a sense of time, a problem similar to the lack of spatial perspective. Time seems to pass very slowly, akin to an LSD experience. The lack of time and space perspective also leads to a distorted sense of velocity. For example, one could be inching along ever so slowly in reality, yet it would seem as if one were sprinting uncontrollably along a moving walkway, leading to severe, overwhelming disorientation.
Sufferers of Alice in Wonderland Syndrome can often experience paranoia as a result of disturbances in sound perception. This can include amplification of soft sounds or misinterpretation of common sounds.
In addition, some people may, in conjunction with a high fever, experience more intense and overt hallucinations, seeing things that are not there and misinterpreting events and situations. Less frequent symptoms sometimes described in Alice in Wonderland Syndrome patients include loss of limb control and dis-coordination, memory loss, lingering touch and sound sensations, and emotional instability.
It has been noted that patients are often reluctant to describe their symptoms due to fear of being labeled with a psychiatric disorder. It is usually easy to rule out psychosis as those with Alice in Wonderland Syndrome are typically aware that their hallucinations and distorted perceptions are not ‘real’, and they have not lost touch with reality. Furthermore, younger patients who frequently experience Alice in Wonderland syndrome may struggle to describe their unusual symptoms, and thus, it is recommended to encourage children to draw their visual illusions during episodes. It appears that the symptoms of AiWS do not change in severity over the course of the syndrome, and though the symptoms may acutely impact the patient’s life, Alice in Wonderland syndrome typically resolves itself within weeks or months. Furthermore, AiWS symptoms occur transiently during the day for short periods of time, with most patients describing their symptoms as lasting anywhere between 10 seconds to 10 minutes. This, combined with the typically short duration of the syndrome, suggests that Alice in Wonderland Syndrome typically causes a relatively short-term disruption of normal functioning. However, symptoms can be debilitating when experienced, and the individual should exercise caution, for example when driving, as the symptoms can appear rapidly. Symptom severity influences whether or not the individual will be able to hold a job during these periods of misperception.
Come back tomorrow for Part II on Alice in Wonderland!
“Seek immediate care if a hernia bulge turns red, purple or dark or if you notice any other signs or symptoms of a strangulated hernia.
See your doctor if you have a painful or noticeable bulge in your groin on either side of your pubic bone. The bulge is likely to be more noticeable when you’re standing, and you usually can feel it if you put your hand directly over the affected area.”
“The longevity gap is responsible for the striking demographic characteristics of older Americans. More than half of all women older than 65 are widows, and widows outnumber widowers by at least three to one. At age 65, for every 100 American women, there are only 77 men. Men die younger than women, and they are more burdened by illness during life. They fall ill at a younger age and have more chronic illnesses than women. For example, men are nearly 10 times more likely to get inguinal hernias than women, and five times more likely to have aortic aneurysms. American men are about four times more likely to be hit by gout; they are more than three times more likely than women to develop kidney stones, to become alcoholics, or to have bladder cancer. And they are about twice as likely to suffer from emphysema or a duodenal ulcer. Although women see doctors more often than men, men cost our society much more for medical care beyond age 65.”.
Harvard Health Publishing – Harvard Medical School (https://www.health.harvard.edu)
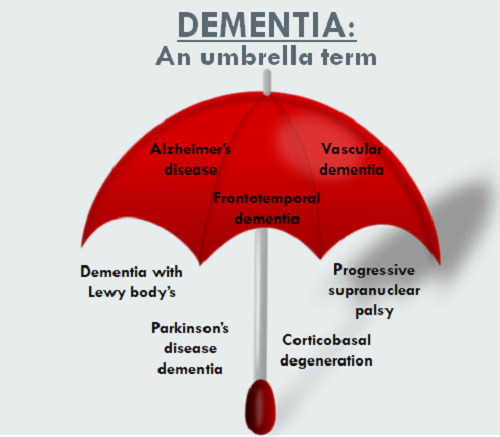
“Alzheimer’s worsens over time. Alzheimer’s is a progressive disease, where dementia symptoms gradually worsen over a number of years. Alzheimer’s is a type of dementia that affects memory, thinking and behavior. Symptoms eventually grow severe enough to interfere with daily tasks. Alzheimer’s Disease is the most common cause of dementia. Alzheimer’s disease accounts for 60-80% of dementia cases.”.
Here is a summary of the seven stages of Alzheimer’s based on Dr. Resiberg’s system:
Stage 1: No Impairment
During this stage, Alzheimer’s is not detectable and no memory problems or other symptoms of dementia are evident.
Stage 2: Very Mild Decline
The senior may notice minor memory problems or lose things around the house, although not to the point where the memory loss can easily be distinguished from normal age-related memory loss. The person will still do well on memory tests and the disease is unlikely to be detected by loved ones or physicians.
Stage 3: Mild Decline
At this stage, the family members and friends of the senior may begin to notice cognitive problems. Performance on memory tests are affected and physicians will be able to detect impaired cognitive function.
People in stage 3 will have difficulty in many areas including:
Finding the right word during conversations
Organizing and planning
Remembering names of new acquaintances
People with stage three Alzheimer’s may also frequently lose personal possessions, including valuables.
Stage 4: Moderate Decline
In stage four of Alzheimer’s, clear-cut symptoms of the disease are apparent. People with stage four of Alzheimer’s:
Have difficulty with simple arithmetic
Have poor short-term memory (may not recall what they ate for breakfast, for example)
Inability to manage finance and pay bills
May forget details about their life histories
Stage 5: Moderately Severe Decline
During the fifth stage of Alzheimer’s, people begin to need help with many day-to-day activities. People in stage five of the disease may experience:
Difficulty dressing appropriately
Inability to recall simple details about themselves such as their own phone number
Significant confusion
On the other hand, people in stage five maintain functionality. They typically can still bathe and toilet independently. They also usually still know their family members and some detail about their personal histories, especially their childhood and youth.
Stage 6: Severe Decline
People with the sixth stage of Alzheimer’s need constant supervision and frequently require professional care. Symptoms include:
Confusion or unawareness of environment and surroundings
Inability to recognize faces except for the closest friends and relatives
Inability to remember most details of personal history
Loss of bladder and bowel control
Major personality changes and potential behavior problems
The need for assistance with activities of daily living such as toileting and bathing
Wandering
Stages 7: Very Severe Decline
Stage seven is the final stage of Alzheimer’s. Because the disease is a terminal illness, people in stage seven are nearing death. In stage seven of the disease, people lose the ability to communicate or respond to their environment. While they may still be able to utter words and phrases, they have no insight into their condition and need assistance with all activities of daily living. In the final stages of Alzheimer’s, people may lose their ability to swallow.