The nervous system consists of the brain, spinal cord, sensory organs, and all of the nerves that connect these organs with the rest of the body. Together, these organs are responsible for the control of the body and communication among its parts.
What are the parts of the nervous system?
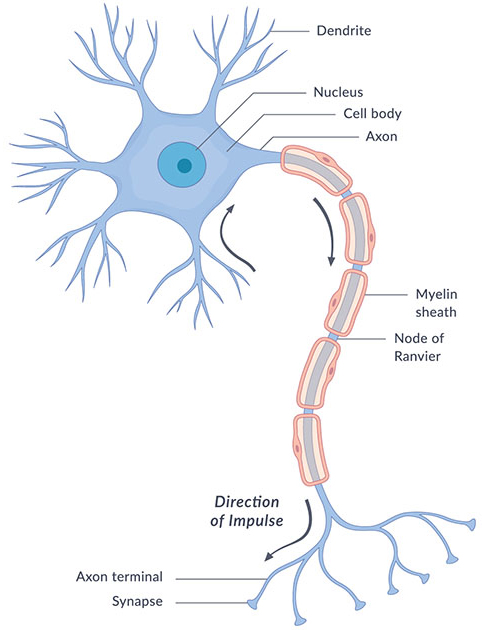
The nervous system transmits signals between the brain and the rest of the body, including internal organs. In this way, the nervous system’s activity controls the ability to move, breathe, see, think, and more.
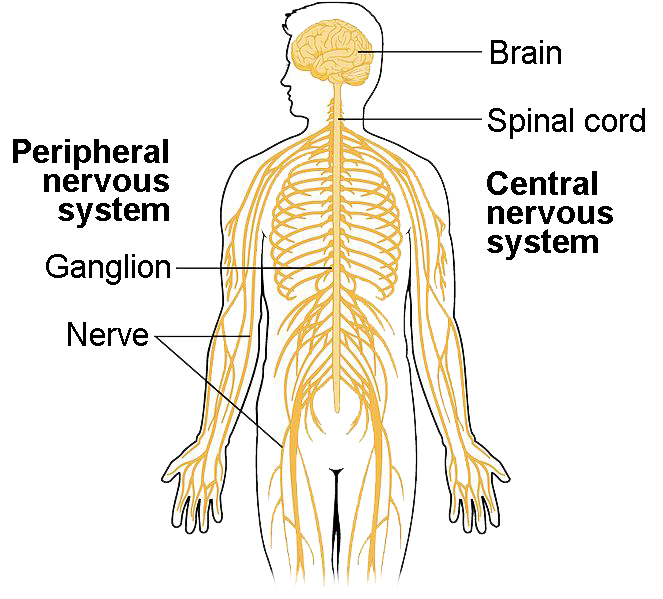
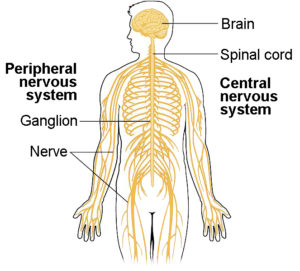
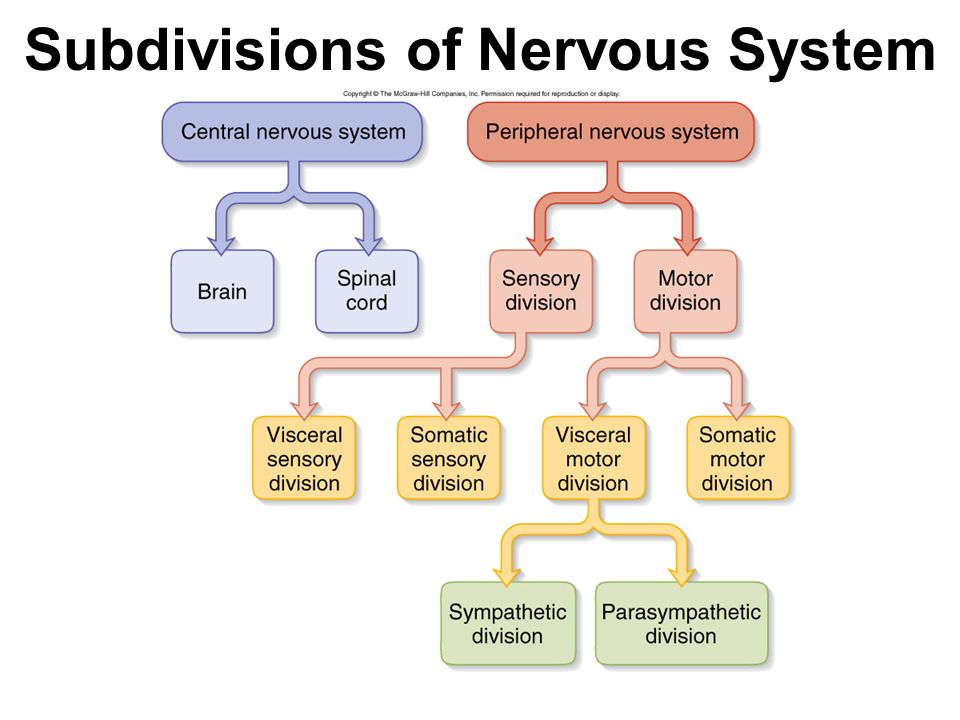
The nervous system is a complex, sophisticated system that regulates and coordinates body activities. It is made up of two major divisions or has 2 main parts, including the following:
1-CNS (Central Nervous System) and 2-PNS (Peripheral Nervous System)
- 1-Central nervous system. This consists of the brain and spinal cord. The central nervous system (defined as the brain and spinal cord) is usually considered to have seven basic parts: the spinal cord, the medulla, the pons, the cerebellum, the midbrain, the diencephalon, and the cerebral hemispheres
SUBDIVISION OF THE CENTRAL NERVOUS SYSTEM; CRANIAL NERVES:
Table 1.1The Cranial Nerves and Their Primary Functions
| Cranial nerve |
Name |
Sensory and/or motor |
Major function |
Location of cells whose axons form the nerve |
Clinical test of function |
| I |
Olfactory nerve |
Sensory |
Sense of smell |
Nasal epithelium |
Test sense of smell with standard odor |
| II |
Optic nerve |
Sensory |
Vision |
Retina |
Measure acuity and integrity of visual field |
| III |
Oculomotor nerve |
Motor |
Eye movements; papillary constriction and accommodation; muscles of eyelid. |
Oculomotor nucleus in midbrain; Edinger-Westphal nucleus in midbrain |
Test eye movements (patient can’t look up, down, or medially if nerve involved); look for ptosis, pupillary dilation |
| IV |
Trigeminal nerve |
Motor |
Eye movements |
Trochlear nucleus in midbrain |
Can’t look downward when eye abducted |
| V |
Trochlear nerve |
Sensory and motor |
Somatic sensation from face, mouth, cornea; muscles of mastication |
Trigeminal motor nucleus in pons; trigeminal sensory ganglion (the gasserian ganglion) |
Test sensation on face; palpate masseter muscles and temporal muscle |
| VI |
Abducens nerve |
Motor |
Eye movements |
Abducens nucleus in midbrain |
Can’t look laterally |
| VII |
Facial nerve |
Sensory and motor |
Controls the muscles of facial expression; taste from anterior tongue; lacrimal and salivary glands |
Facial motor nucleus; superior salivatory nuclei in pons; trigeminal (gasserian) ganglion |
Test facial expression plus taste on anterior tongue |
| VIII |
Auditory/vestibular nerve |
Sensory |
Hearing;sense of balance |
Spiral ganglion; vestibular (Scarpa’s) ganglion |
Test audition with tuning fork; vestibular function with caloric test |
| IX |
Glossopharyngeal nerve |
Sensory and motor |
Sensation from pharynx; taste from posterior tongue; carotid baroreceptors |
Nucleus ambiguus; inferior salivatory |
Test swallowing; pharyngeal gag reflex |
| X |
Vague nerve |
Sensory and motor |
Autonomic functions of gut; sensation from pharynx; muscles of vocal cords; swallowing |
Dorsal motor nucleus of vagus; vagal nerve ganglion |
Test above plus hoarseness |
| XI |
Accessory nerve |
Motor |
Shoulder and neck muscles |
Spinal accessory nucleus; nucleus ambiguus; intermediolateral column of spinal cord |
Test sternocleidomastoid and trapezius muscles |
| XII |
Hypoglossal nerve |
Motor |
Movements of tongue |
Hypoglossal nucleus of medulla |
Test deviation of tongue during protrusion (points to side of lesion) |
- 2-Peripheral nervous system. This consists of all other neural elements, including the peripheral nerves and the autonomic nerves. This makes up a large division of the enteric nervous system which we will get into later. Also your peripheral nervous system contains your:
- Somatic nervous system, which guides your voluntary movements. The somatic nervous system is a component of the peripheral nervous system associated with the voluntary control of the body movements via the use of skeletal muscles.
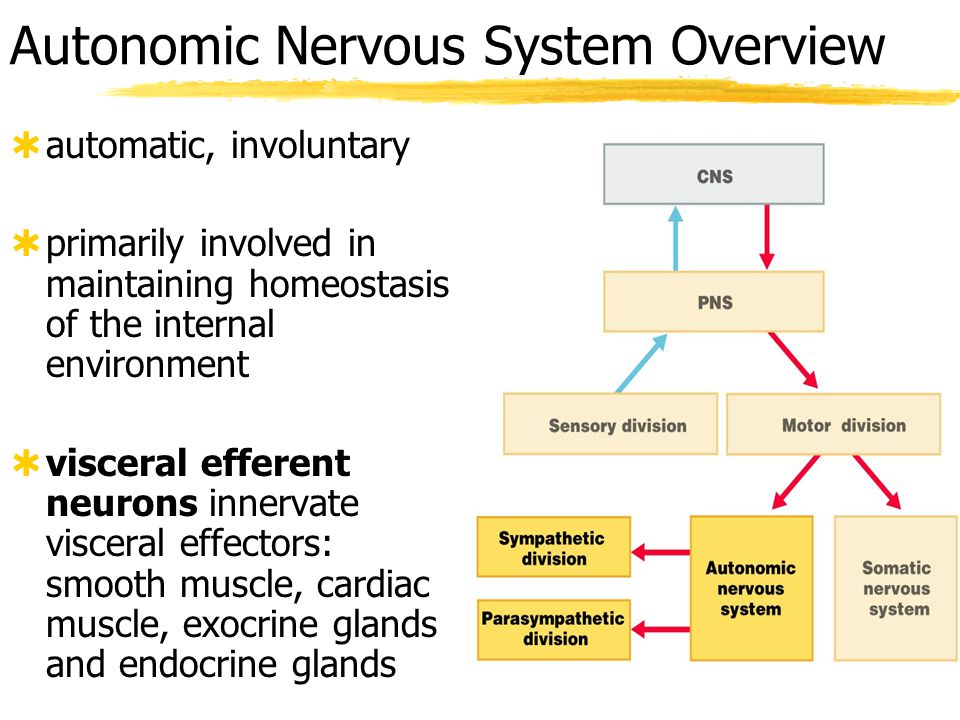
- Autonomic nervous system, which controls the activities you do without thinking about them; involuntary control (ex. Breathing). Autonomic Nervous System further breaks down into
.
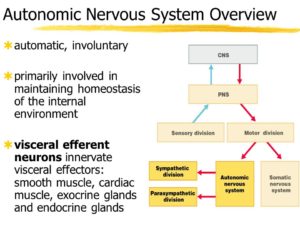
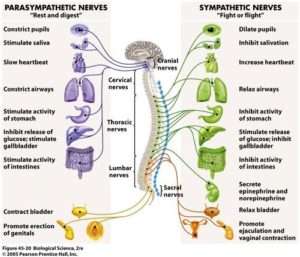
The autonomic nervous system has three branches:
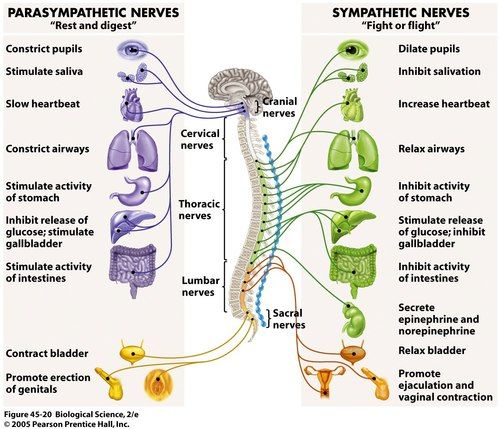
1-The Sympathetic Nervous System 2-The Parasympathetic Nervous System and
The parasympathetic nervous system is able to stimulate the enteric nerves in order to increase enteric function. The parasympathetic enteric neurons function in defecation and provide a rich nerve supply to the sigmoid colon, the rectum, and the anus.
3-The Enteric Nervous System. Some textbooks do not include the enteric nervous system as part of this system.
3-The enteric nervous system (ENS) is a large division of the peripheral nervous system (PNS) that can control gastrointestinal behaviour independently of central nervous system (CNS) input. Mammalian neurons are located in either the CNS (brain and spinal cord) or PNS (cells with soma outside the brain and spinal cord).
The enteric nervous system (ENS) is a web of sensory neurons, motor neurons, and interneurons embedded in the wall of the gastrointesinal system, stretching from the lower third of the esophagus right through to the rectum.
The enteric nervous system (ENS) is known as the “second brain” or the brain in the gut because it can operate independently of the brain and spinal cord, the central nervous system (CNS). It has also been called the “first brain” based on evidence suggesting that the ENS evolved before the CNS.
So in review the makeup of the Autonomic Nervous System = Parasympathetic, Sympathetic & Enteric Nervous Systems. Further subdividing down to the somatic and visceral nervous systems.
Somatic sensory input comes from the receptors of the eyes, ears, nose, tongue, and skin. These organs transmit information we associate with the five senses; making up the somatic nervous system in the peripheral nervous system.
Visceral sensory input comes from (surprise!) the viscera, or internal organs; making up the visceral nervous system in the peripheral nervous system.