“STDs such as syphilis and HIV can have severe consequences if left untreated. Even common diseases such as gonorrhea and chlamydia can cause problems if undiagnosed for long periods of time.”
Centers for Disease Control and Prevention (CDC)
“Men who have sex with men (MSM) have increased rates of human immunodeficiency virus (HIV) infection and sexually transmitted diseases (STDs) compared with demographically matched controls. The reasons for the disproportionate infection burden are complex, including biological, behavioral, and sociocultural factors.HIV and syphilis may often be coprevalent among MSM. ”

The term “men who have sex with men” (MSM) describes a heterogeneous group of men who have varied behaviors, identities, and health-care needs. Some MSM are at high risk for HIV infection and other viral and bacterial STDs because MSM may practice anal sex, and the rectal mucosa is uniquely susceptible to certain STD pathogens. In addition, multiple sex partners, substance use, and sexual network dynamics of MSM increase risk for HIV and STDs in this population. The frequency of unsafe sexual practices and the reported rates of bacterial STDs and incident HIV infection declined substantially in MSM from the 1980s through the mid-1990s. However, since that time, increased rates of early syphilis (primary, secondary, or early latent), gonorrhea, and chlamydial infection and higher rates of sexual risk behaviors have been documented among MSM in the United States and virtually all industrialized countries.
Approximately two thirds of the cases of primary and secondary syphilis diagnoses in the United States are in MSM, particularly those in ethnic minority groups. Increased syphilis screening in MSM demonstrated a doubling of early syphilis detection; however, 71% of the syphilis diagnoses occurred when the patient sought care for symptoms . Acute HIV infection has been associated with a recent or concurrent STD, including syphilis, among men at a municipal STD clinic. Factors associated with increases in syphilis among MSM have included substance abuse (e.g., methamphetamine), having multiple anonymous partners, and seeking sex partners through the internet.
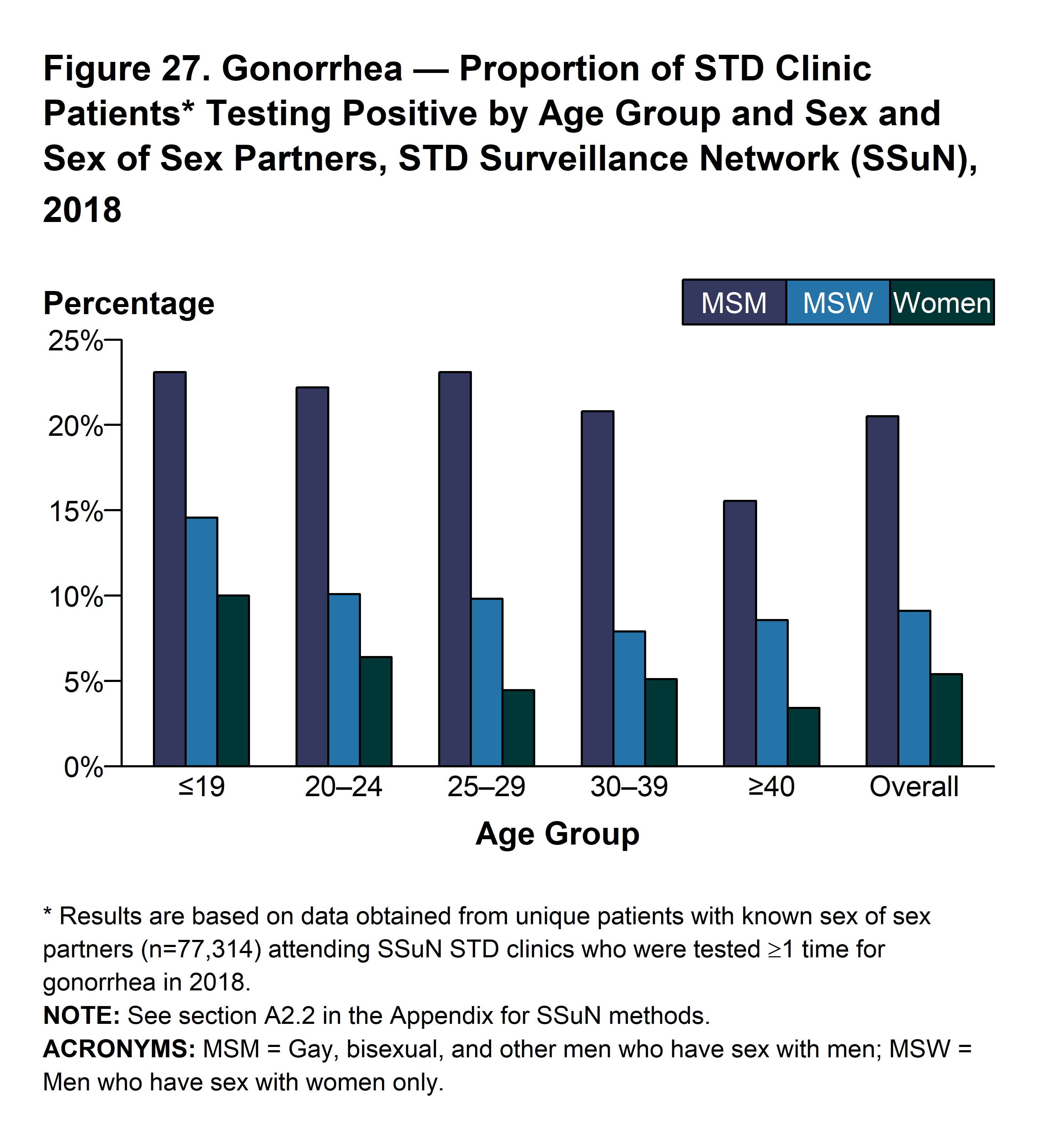
Gonococcal infection in MSM has been associated with similar risk factors, including having multiple anonymous partners and abuse of substances, particularly crystal methamphetamine. Rectal gonococcal rates are increasing among MSM with HIV infection, underscoring the importance of obtaining an accurate, current sexual history and asking about correlates of increased risk (e.g., anonymous sex and substance use). Insertive oral sex has been associated with urethral gonorrhea acquisition.
MSM remain at disproportionate risk for HIV acquisition and transmission in the United States, particularly those who are black or Hispanic. Factors that increase the risk for HIV infection in MSM include either receptive or insertive anal sex without a condom, having another STD, having sex with anonymous partners without a condom, and using methamphetamines or drugs that enhance sexual performance.
Clinicians should routinely ask sexually active MSM about symptoms consistent with common STDs, including urethral discharge, dysuria, genital and perianal ulcers, regional lymphadenopathy, skin rash, and anorectal symptoms consistent with proctitis (e.g., discharge and pain on defecation or during anal intercourse) and then perform appropriate diagnostic testing. In addition, providers should offer evidence-based counseling on safer sex using interventions that have been demonstrated to decrease STD incidence in clinical-care settings.
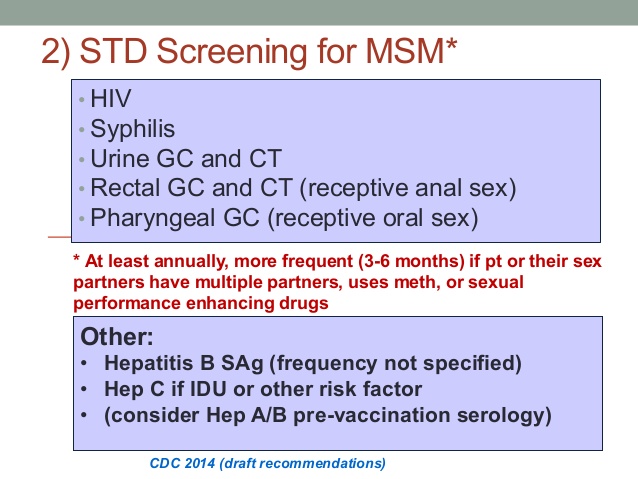
The following screening tests should be performed at least annually for sexually active MSM, including those with HIV infection.
MSM with HIV infection are also at risk for STDs. Data from a study of 557 adults with HIV infection receiving primary care in four U.S. cities demonstrate that 13% had STD at study enrollment, and 7% had incident STD at 6 months; among MSM with HIV infection, STD incidence was 20%. Excluding trichomoniasis, 94% of incident STDs were diagnosed in MSM. All MSM with HIV infection entering care should be screened for gonorrhea and chlamydia at appropriate anatomic sites of exposure, as well as for syphilis. The frequency of follow-up testing might be dictated by subsequent behavior; screening is recommended annually, at a minimum, to include syphilis serologic testing and chlamydia and gonorrhea screening at exposed anatomic sites). STD screening rates in HIV clinics have been suboptimal. In one study involving eight U.S. cities, although syphilis testing was provided to most MSM with HIV infection, <10% were screened for extra-genitourinary gonorrhea or chlamydia, and <20% provided the urine or urethral specimens needed for testing. More frequent STD screening (i.e., for syphilis, gonorrhea, and chlamydia) at 3–6-month intervals is indicated for MSM, including those with HIV infection if risk behaviors persist or if they or their sexual partners have multiple partners. Evaluation for HSV-2 infection with type-specific serologic tests also can be considered if infection status is unknown in persons with previously undiagnosed genital tract infection.
HPV infection and HPV-associated conditions (e.g., anogenital warts and anal squamous intraepithelial lesions) are highly prevalent among MSM. The quadrivalent vaccine is recommended routinely for MSM through age 26 years; the efficacy of this vaccine in preventing HPV associated diseases in men aged >26 years is unknown.
Data are insufficient to recommend routine anal-cancer screening with anal cytology in persons with HIV infection or HIV-negative MSM. More evidence is needed concerning the natural history of anal intraepithelial neoplasia, the best screening methods and target populations, safety of and response to treatments, and other programmatic considerations before screening can be routinely recommended. However, some clinical centers perform anal cytology to screen for anal cancer among high-risk populations (e.g., persons with HIV infection and MSM), followed by high-resolution anoscopy for those with abnormal cytologic results (e.g., ASC-US).
“While sexually transmitted diseases (STDs) affect individuals of all ages, STDs take a particularly heavy toll on young people. CDC estimates that youth ages 15-24 make up just over one quarter of the sexually active population, but account for half of the 20 million new sexually transmitted infections that occur in the United States each year.”
Centers for Disease Control and Prevention of disease
“The most destructive form of alcoholism is chronic alcoholism, an emotionally, socially and physically devastating disease. Alcoholism emerges from alcohol abuse, when there’s a pattern of drinking despite negative consequences. Alcoholism and alcohol abuse are both categorized as alcohol use disorders—affecting people of all ages and stages of life.”
Hazelden Betty Ford Foundation
“Alcohol use disorder (which includes a level that’s sometimes called alcoholism) is a pattern of alcohol use that involves problems controlling your drinking, being preoccupied with alcohol, continuing to use alcohol even when it causes problems, having to drink more to get the same effect, or having withdrawal symptoms when you rapidly decrease or stop drinking”
MAYO CLINIC
“A congregate setting is an environment where a number of people reside, meet or gather in closeproximity for either a limited or extended period of time.”
NYC.gov
“After the peak of illness during the second wave had come and gone in the United States. From April 12, 2009 to April 10, 2010, CDC estimated there were 60.8 million cases (range: 43.3-89.3 million), 274,304 hospitalizations (range: 195,086-402,719), and 12,469 deaths (range: 8868-18,306) in the United States due to the (H1N1)pdm09 virus.”
Centers for Disease Prevention and Control (CDC)
The coronavirus has upended countless lives here at home and around the world. We’ve all become too familiar with new terms — shelter in place, flatten the curve, social distancing. The stock market is bouncing wildly. Just this week we saw the greatest number of unemployment applications in our nation’s history. And there’s still no toilet paper at the grocery store, if you can even go to the grocery store. So are you feeling stressed yet? Anxious? At your wits’ end because you’re trying to telework and the kids are making noise in the next room? And will someone please walk the dog?
Many people are reckoning with individual losses, including illness and death due to the novel coronavirus, or loss of employment as a result of economic upheaval. But even people who haven’t lost anything so concrete as a job or a loved one are affected. Its makes you think is the depression going to happen again since hitory rpeats itself. Look at Pandemics, are last one was in 2009-2010 when the President Obama was in office and we had more deaths than but it wasn’t majority in NYC. The Corona 19 will probably over ride in deaths but we are far from the end. Keep in mind H1N1 after the peak of illness during the second wave had come and gone in the United States. From April 12, 2009 to April 10, 2010, CDC estimated there were 60.8 million cases (range: 43.3-89.3 million), 274,304 hospitalizations (range: 195,086-402,719), and 12,469 deaths (range: 8868-18,306) in the United States due to the (H1N1)pdm09 virus.
Things should get better based on history and hopefully close in the future we will all get on a more normal working schedule again. We will get through this and maybe our country and cities might consider stricter regulations with traveling in and out of America, better control of city populations in the U.S., and cleaner cities. Since all these aspects play an impact on why Corona virus ended up in America and where the high amount of cases are located.
“Diagnosing ASD can be difficult since there is no medical test, like a blood test, to diagnose the disorders. Doctors look at the child’s behavior and development to make a diagnosis.
ASD can sometimes be detected at 18 months or younger. By age 2, a diagnosis by an experienced professional can be considered very reliable.1 However, many children do not receive a final diagnosis until much older. This delay means that children with ASD might not get the early help they need.”
“Autism is a complex, lifelong developmental disability that typically appears during early childhood and can impact a person’s social skills, communication, relationships, and self-regulation. Autism is defined by a certain set of behaviors and is a “spectrum condition” that affects people differently and to varying degrees.
While there is currently no known single cause of autism, early diagnosis helps a person receive the support and services that they need, which can lead to a quality life filled with opportunity.”
Autism Society (www.autism-society.org)