Treatment
Your thyroid cancer treatment options depend on the type and stage of your thyroid cancer, your overall health, and your preferences.
Most cases of thyroid cancer can be cured with treatment.
Surgery
Most people with thyroid cancer undergo surgery to remove all or most of the thyroid. Operations used to treat thyroid cancer include:
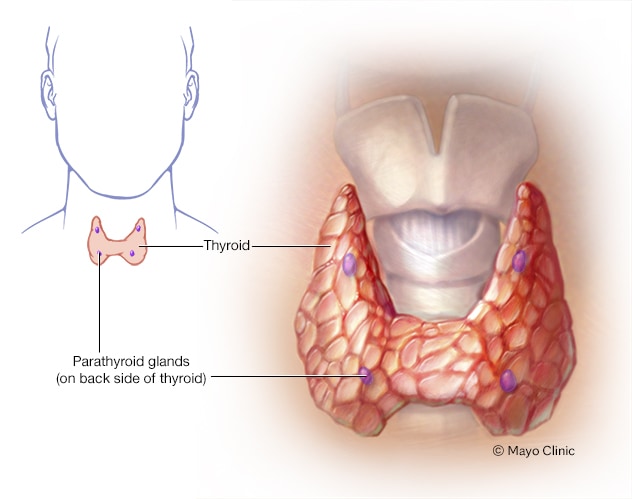
- Removing all or most of the thyroid (thyroidectomy). In most cases, doctors recommend removing the entire thyroid in order to treat thyroid cancer. Your surgeon makes an incision at the base of your neck to access your thyroid.In most cases, the surgeon leaves small rims of thyroid tissue around the parathyroid glands to reduce the risk of parathyroid damage. Sometimes surgeons refer to this as a near-total thyroidectomy.
- Removing lymph nodes in the neck. When removing your thyroid, the surgeon may also remove enlarged lymph nodes from your neck and test them for cancer cells.
- Removing a portion of the thyroid (thyroid lobectomy). In certain situations where the thyroid cancer is very small, your surgeon may recommend removing only one side (lobe) of your thyroid.
Thyroid surgery carries a risk of bleeding and infection. Damage can also occur to your parathyroid glands during surgery, which can lead to low calcium levels in your body. There’s also a risk of accidental damage to the nerves connected to your vocal cords, which can cause vocal cord paralysis, hoarseness, soft voice or difficulty breathing.
Thyroid hormone therapy
After thyroidectomy, you’ll take the thyroid hormone medication levothyroxine (Levoxyl, Synthroid, others) for life.
This medication has two benefits: It supplies the missing hormone your thyroid would normally produce, and it suppresses the production of thyroid-stimulating hormone (TSH) from your pituitary gland. High TSH levels could conceivably stimulate any remaining cancer cells to grow.
You’ll likely have blood tests to check your thyroid hormone levels every few months until your doctor finds the proper dosage for you. Blood tests may continue annually.
Radioactive iodine
Radioactive iodine treatment uses large doses of a form of iodine that’s radioactive.
Radioactive iodine treatment is often used after thyroidectomy to destroy any remaining healthy thyroid tissue, as well as microscopic areas of thyroid cancer that weren’t removed during surgery. Radioactive iodine treatment may also be used to treat thyroid cancer that recurs after treatment or that spreads to other areas of the body.
Radioactive iodine treatment comes as a capsule or liquid that you swallow. The radioactive iodine is taken up primarily by thyroid cells and thyroid cancer cells, so there’s a low risk of harming other cells in your body.
Side effects may include:
- Nausea
- Dry mouth
- Dry eyes
- Altered sense of taste or smell
- Fatigue
Most of the radioactive iodine leaves your body in your urine in the first few days after treatment. You’ll be given instructions for precautions you need to take during that time to protect other people from the radiation. For instance, you may be asked to temporarily avoid close contact with other people, especially children and pregnant women.
External radiation therapy
Radiation therapy can also be given externally using a machine that aims high-energy beams, such as X-rays and protons, at precise points on your body (external beam radiation therapy). This treatment is typically administered a few minutes at a time, five days a week, for about five weeks. During treatment, you lie still on a table while a machine moves around you.
External beam radiation therapy may be an option if you can’t undergo surgery and your cancer continues to grow after radioactive iodine treatment. Radiation therapy may also be recommended after surgery if there’s an increased risk that your cancer will recur.
Chemotherapy
Chemotherapy is a drug treatment that uses chemicals to kill cancer cells. Chemotherapy is typically given as an infusion through a vein. The chemicals travel throughout your body, killing quickly growing cells, including cancer cells.
Chemotherapy is not commonly used in the treatment of thyroid cancer, but it may benefit some people who don’t respond to other therapies. For people with anaplastic thyroid cancer, chemotherapy may be combined with radiation therapy.
Injecting alcohol into cancers
Alcohol ablation involves injecting small thyroid cancers with alcohol using imaging such as ultrasound to ensure precise placement of the injection. This treatment is helpful for treating cancer that occurs in areas that aren’t easily accessible during surgery. Your doctor may recommend this treatment if you have recurrent thyroid cancer limited to small areas in your neck.
Targeted drug therapy
Targeted drug therapy uses medications that attack specific vulnerabilities in your cancer cells.
Targeted drugs used to treat thyroid cancer include:
- Cabozantinib (Cometriq)
- Sorafenib (Nexavar)
- Vandetanib (Caprelsa)
These drugs target the signals that tell cancer cells to grow and divide. They’re used in people with advanced thyroid cancer.
Supportive (palliative) care
Palliative care is specialized medical care that focuses on providing relief from pain and other symptoms of a serious illness. Palliative care specialists work with you, your family and your other doctors to provide an extra layer of support that complements your ongoing care. Palliative care can be used while undergoing other aggressive treatments, such as surgery, chemotherapy or radiation therapy.
When palliative care is used along with all of the other appropriate treatments, people with cancer may feel better and live longer.
Palliative care is provided by a team of doctors, nurses and other specially trained professionals. Palliative care teams aim to improve the quality of life for people with cancer and their families. This form of care is offered alongside curative or other treatments you may be receiving.