Ventricular Rhythms Part III
 PVC
PVC 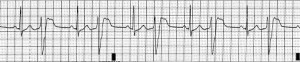 PVC after every one normal beat
PVC after every one normal beat
 BIGEMINI-PVC AFTER 2 NORMAL BEATS (TRIGEMINI-AFTER 3 BEATS)
BIGEMINI-PVC AFTER 2 NORMAL BEATS (TRIGEMINI-AFTER 3 BEATS)
 QUADROGEMINI -AFTER 4 NORMAL BEATS
QUADROGEMINI -AFTER 4 NORMAL BEATS
 40 to 60 beats is just Idioventricular Rhythm,
40 to 60 beats is just Idioventricular Rhythm, 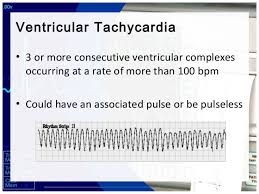 Monomorphic V-Tac
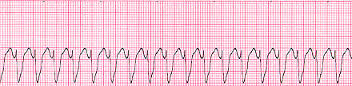
Monomorphic V-Tac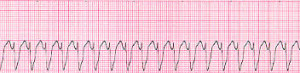
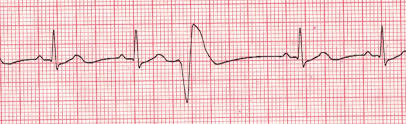
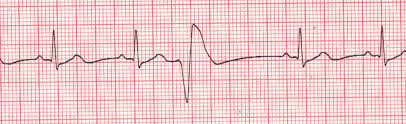
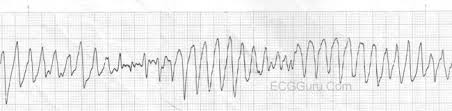
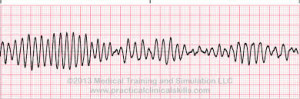
 Below is 2 views of Torsades de Pointes (article describes)
Below is 2 views of Torsades de Pointes (article describes)
 &
& 
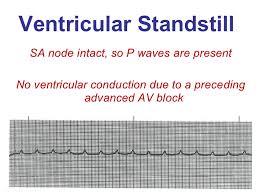
When the atriums aren’t working as the natural pacemaker, called the SA Node located in the top L corner of the right atrium. The atriums that took over for the sinus node now fail don’t work so now the ventricles take over and the rhythms of all ventricle rhythms will show on the EKG which present NO p waves since the atriums are not working so no p wave is involved but we have QRS waves but their wide in measurement because the rhythm starts in the ventricles. The rhythms are PVC (Premature Ventricular Contractions), Idioventricular Rhythm, Ventricular tachycardia (Monomorphic and Polymorphic-rhythm getting more irregular. When regular and monomorphic=looking identical with every ventricular beat or contraction as opposed to polymorphic=not looking identical each contraction but each one is a ventricular contraction), Torsades De Pointes Ventricular Tachycardia (the rhythm starts upright but turns upside down but each contraction without a p wave and a wide contraction meaning a ventricular contraction), and Ventricular Fibrillation, to asystole.
Here’s what they look like:
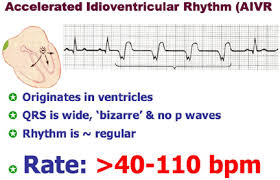
Accelerated Idioventricular Rhythm
Accelerated idioventricular rhythm occurs when three or more ventricular escape beats appear in a sequence. Heart rate will be 50-100 bpm. The QRS complex will be wide (0.12 sec. or more).
A regular QRS measures less than 0.12 which is with all atriums rhythms.
Asystole
Asystole is the state of no cardiac electrical activity and no cardiac output. Immediate action is required.
Idioventricular Rhythm
Idioventricular rhythm is a slow rhythm of under 50 bpm. It indicates that then ventricules are producing escape beats.
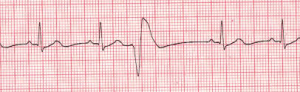
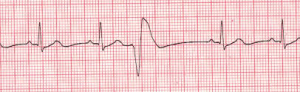
Premature Ventricular Complex
Premature ventricular complexes (PVCs) occur when a ventricular site generates an impulse. This happens before the next regular sinus beat. Look for a wide QRS complex, equal or greater than 0.12 sec. The QRS complex shape can be bizarre. The P wave will be absent.
Premature Ventricular Complex – Bigeminy a QRS after every 2 regular beats
Premature Ventricular Complex – Trigeminy a QRS after every 3 regular beats
Premature Ventricular Complex – Quadrigeminy a QRS after every 4 regular beats
Ventricular Fibrillation
Ventricular fibrillation originates in the ventricules and it chaotic. No normal EKG waves are present. No heart rate can be observed. Ventricular fibrillation is an emergency condition requiring immediate action.
Ventricular Tachycardia
A sequence of three PVCs in a row is ventricular tachycardia. The rate will be 120-200 bpm. Ventricular Tachycardia has two variations, monomorphic and polymorphic. These variations are discussed separately.
Ventricular Tachycardia Monomorphic
Monomorphic ventricular tachycardia occurs when the electrical impulse originates in one of the ventricules. The QRS complex is wide. Rate is above 100 bpm.
Ventricular Tachycardia Polymorphic
Polymorphic ventricular tachycardia has QRS complexes that very in shape and size. If a polymorphic ventricular tachycardia has a long QT Interval, it could be Torsade de Pointes.
Torsade de Pointes
Torsade de Pointes is a special form of ventricular tachycardia. The QRS complexes vary in shape and amplitude and appear to wind around the baseline.
Ventricular ending line needs to be treated stat to be switched back to atrial since the heart is missing ½ of the conduction it’s to normally receive from the atriums and if not reversed the heart will go into failure to heart attack or to asystole flat line and go into a cardiac arrest.
With PVCs=Premature Ventricle Contractions asymptomatic we just closely monitor the pt and telemetry the pt is on. Now a pt with PVCs and symtomatic usually meds with 0xygen (sometimes 02 alone resolves it but other times with meds) but if it gets worse into V Tachycardia the treatment is below.
Idioventricular Rhythm is usually with a slow brady pulse and needs meds. AIVR is usually hemodynamically tolerated and self-limited; thus, it rarely requires treatment.
Occasionally, patients may not tolerate AIVR due to (1) loss of atrial-ventricular synchrony, (2) relative rapid ventricular rate, or (3) ventricular tachycardia or ventricular fibrillation degenerated from AIVR (extremely rare). Under these situations, atropine can be used to increase the underlying sinus rate to inhibit AIVR.
Other treatments for AIVR, which include isoproterenol, verapamil, antiarrhythmic drugs such as lidocaine and amiodarone, and atrial overdriving pacing are only occasionally used today.
Patients with AIVR should be treated mainly for its underlying causes, such as digoxin toxicity, myocardial ischemia, and structure heart diseases. Beta-blockers are often used in patients with myocardial ischemia-reperfusion and cardiomyopathy
With Ventricular rhythms with fast pulse over 100 with symptomatic signs for the patient we may use as simple as valsalva pressure on the neck that medical staff only do but when pt is in asymptomatic (no symptoms) Ventricular Tachycardia (V-Tac) to even medications but when symptomatic if in V-Tac start cardioversion with a pulse if no pulse called pulseless V-Tac we use a defibrillator since there is no pulse there is no QRS to pace with in having the shock hit at the R wave, why? NO PULSE.
Treatment for Torsade de Pointes is Magnesium deficiency and Mag. Supplement given IV 2gms. Usually effective but if necessary the same as above as directed for it with a pulse or the other V Tac. (without a pulse)-See above.
Ventricular Fibrillation is when the ventricles are just quivering and the atriums in any ventricular rhythm doing nothing. The pt needs CPR and ASAP a defibrillator in hopes the shock will knock the rhythm back to a normal sinus or some form of a real rhythm.
Asystole which is a straight line, no pulse and this is CPR with epinephrine or Vasopressin 40 for only the replacement of the 1st or 2nd dose of Epinephrine 1mg. This is given 3-5 minutes (epinephrine). No defibrillation since no pulse. A rhythm may come back and if not the MD will call when CPR stops. Asystole is hard to resolve in most cases highier probability of resolution if in a hospital where close monitoring is done and its detected quicker.
The PURPOSE to all treating rhythms for all patients to the best optimal rhythm they can live with and hopefully reaching the best NSR-Normal Sinus Rhythm is give effective oxygen perfusion to the heart to allow it to do its function and get good amounts of oxygen to all our tissues to keep us alive. A human without oxygen or low oxygen to their tissues or any tissue is starvation to the tissues (in general) or to a tissue (Ex. Diabetic the foot to lack of 02 to cyanotic purple tissue to necrotic black tissue=dead to amputated since the tissue is dead.).