How is Spina Bifida Diagnosed:
In most cases, spina bifida is diagnosed before birth (prenatal). However, some mild cases may go unnoticed until after birth (postnatal). Very mild forms of spinal bifida are found when doing tests for other conditions or may never be detected.
PRENATAL DIAGNOSED:
The most common screening methods used to look for spina bifida during pregnancy are maternal serum alpha fetoprotein (MSAFP) screening and fetal ultrasound. A doctor can also perform an amniocentesis test.
- Maternal serum alpha fetoprotein (MSAFP) screen. At 16 to 18 weeks of pregnancy, a sample of the mother’s blood is taken to measure the level of a protein called alpha-fetoprotein (AFP), which is made naturally by the fetus and placenta. During pregnancy, a small amount of AFP normally crosses the placenta and enters the mother’s bloodstream. Abnormally high levels of AFP may indicate that the fetus has spina bifida or other neural tube defect. This test is not specific for spina bifida and cannot definitively determine that there is a problem with the fetus. This means that a high AFP level alone is not enough to be sure the fetus has a neural tube defect. If a high level of AFP is detected, the doctor may request additional testing, such as an ultrasound or amniocentesis.
The second trimester MSAFP screen may be performed alone or as part of a larger, multiple-marker screen. Multiple-marker screens can look for neural tube defects and other birth defects, including Down syndrome and other chromosomal abnormalities. First trimester screens for chromosomal abnormalities also exist but signs of spina bifida are not evident until the second trimester when the MSAFP screening is performed.
- Ultrasound. A fetal ultrasound uses high-frequency sound waves to create a picture of the developing baby inside the womb. It is highly accurate in diagnosing some birth defects during pregnancy, including spina bifida. Fetal ultrasound can be performed during the first trimester (usually between 11-14 weeks) and the second trimester (usually at 18-22 weeks), and diagnosis is more accurate during the second trimester.
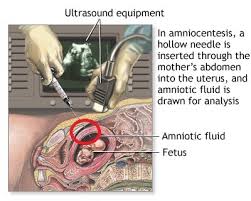
- Amniocentesis. In this test, a doctor removes a sample of the amniotic fluid that surrounds the fetus and tests it for protein levels that may indicate a neural tube defect and genetic disorders.
POSTNATAL DIAGNOSED:
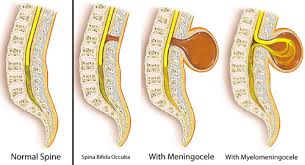
Closed neural tube defects are often recognized at birth due to an abnormal fatty mass, tuft or clump of hair, or a small dimple or birthmark on the skin at the site of the spinal malformation. Spina bifida occulta is usually found when x-rays are done for another reason.
In rare cases, myelomeningocele and meningocele are not diagnosed during routine prenatal tests. The baby will be diagnosed when they are born with a bubble on their back. Babies with myelomeningocele and closed neural tube defects may have muscle weakness in their feet, hips, and legs that result in joint deformities first noticed at birth. Mild cases of spina bifida (occulta, closed neural tube defects) not diagnosed during prenatal testing may be detected postnatally using ultrasound or X-ray imaging to look at the spine.
Doctors may use magnetic resonance imaging (MRI) or a computed tomography (CT) scan to get a clearer view of the spinal cord and vertebrae. To evaluate for hydrocephalus, the doctor will request a head ultrasound, CT or MRI to look for extra cerebrospinal fluid inside the brain.
HOW SPINA BIFIDA CAN BE PREVENTED, THE BEST TREATMENT TO GIVE YOUR BABY; being FOLIC ACID!
Women of childbearing age can reduce their risk of having a child with spina bifida by taking 400 micrograms (mcg) of folic acid every day pre-conception. Because it is water soluble, folic acid does not stay in the body for very long and needs to be taken every day to be effective against neural defects. Since half of all pregnancies in the United States are unplanned, folic acid must be taken whether a woman is planning a pregnancy or not. Research has shown that if all women of childbearing age took a multivitamin with the B-vitamin folic acid, the risk of neural tube defects could be reduced by up to 70%. If you can prevent this the quality life is sure to be the best!
TREATMENTS FOR SPINA BIFIDA:
Some children with myelomeningocele and closed neural tube defects will need surgery to improve the alignment of their feet, legs, or spine. Children with myelomeningocele usually have hydrocephalus and may require surgery to help drain fluid in the brain, such as the placement of a shunt or ETV. Multiple surgeries may be required to replace the shunt, which may become clogged, infected, or disconnected.
Some individuals with myelomeningocele or closed neural tube defects require assistive devices for mobility such as braces, walkers, crutches, or wheelchairs. The location of the defect on the spine often determines the type of assistive devices needed. Children with a defect high on the spine will have little movement of the legs and will use a wheelchair for mobility. Children with a defect lower on the spine usually have more strength in the legs. They may be able to walk independently, or they may use crutches, leg braces, walkers, and wheelchairs depending on the activity. Children with myelomeningocele usually have some degree of delayed mobility, so they are referred to physical therapists early on to maximize their strength and function.
Treatment for bladder and bowel dysfunction typically begins soon after birth. Children with myelomeningocele and some closed neural tube defects have damage to the lowest spinal nerves which control typical bowel and bladder function. Some children may be able to urinate typically, but most will need to drain their bladders with a catheter or thin tube 4-6 times a day to remain dry in between and to prevent kidney damage. Kidneys are monitored closely so that medications or surgeries can be performed to prevent renal failure. To prevent bowel accidents many people with myelomeningocele and closed neural type defects will use rectal medications or large volume enemas to have planned bowel movements. Close follow-up with a spina bifida specialty clinic is recommended to develop a safe bowel and bladder program.
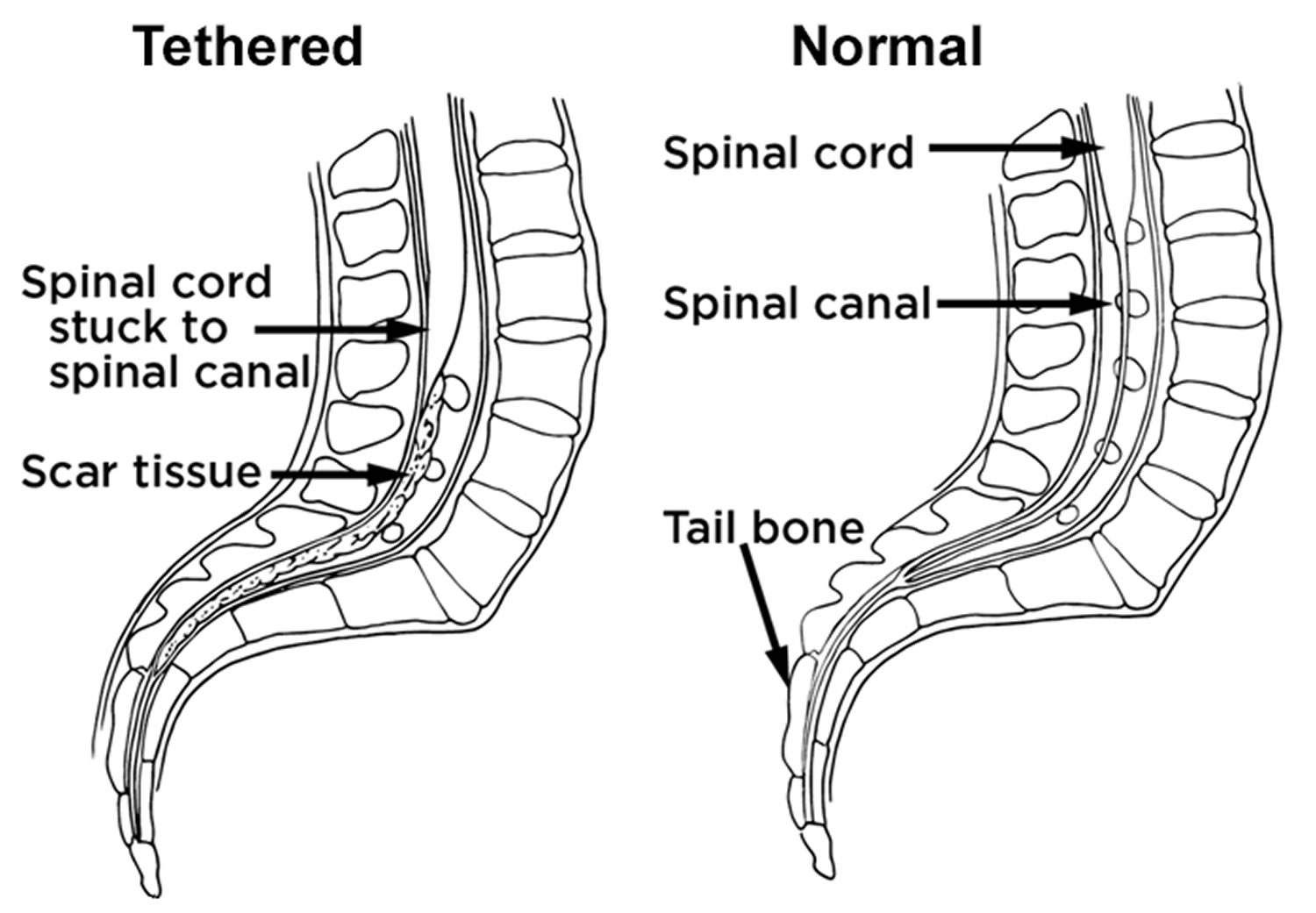
Treatment for progressive tethering of the spinal cord (called tethered cord syndrome) can be treated with surgery to help prevent further neurological deterioration.
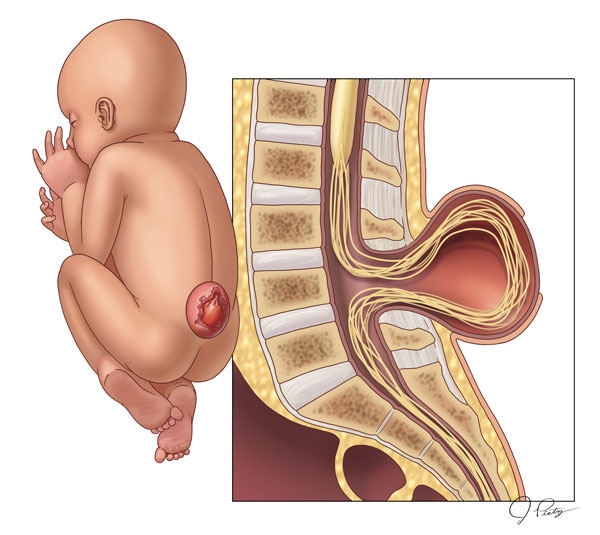 SPINA BIFIDA
SPINA BIFIDA
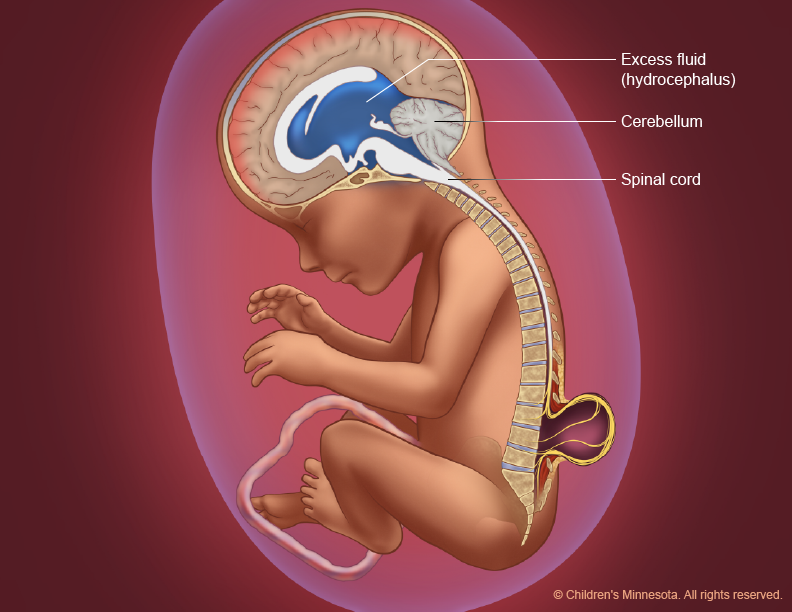
 HYDROCEPHALUS
HYDROCEPHALUS