Diabetes Mellitus (DM) is a complex chronic disease involving disorders in carbohydrate, protein, and fat metabolism and the development of macro-vascular, micro-vascular, neurological complications that don’t occur over a few nights or weeks or months. It is a metabolic disorder in where the pancreas organ ends up causing many disruptions in proper working of our body. The pancreas is both an endocrine and exocrine gland. The problem with diabetes is due to the endocrine part of the pancreas not working properly. More than 1 million islet cells are located throughout the organ. The three types of endocrine cells that the pancreas excretes into our blood stream are alpha, beta, and delta cells. The alpha cells secrete glucagon (stored glucose), beta secrete insulin, and delta secrete gastrin and pancreatic somatostatin. A person with DM has minimal or no beta cells secreted from the pancreas, which shows minimal or no insulin excreted in the person’s bloodstream. Insulin is necessary for the transport of glucose, amino acids, potassium, and phosphate across the cell membrane getting these chemical elements into the cell. When getting these elements into the cells it is like the cell eating a meal and the glucose, being one of the ingredients in the meal, is used for energy=fuel to our body; the glucose inside the cells gets carried to all our tissues in the body to allow the glucose to be utilized into all our tissues so they can do their functions (Ex. Getting glucose into the muscle tissue allows the muscles to have the energy to do the range of motion in letting us do our daily activities of living, like as simple as type or walk). The problem with diabetes is the glucose doesn’t have the insulin being sent into the bloodstream by the pancreas to transfer the glucose across the cell membrane to be distributed as just discussed. Instead what results is a high glucose levels in the blood stream causing hyperglycemia. It should be apparent that when there is a deficit of insulin, as in DM, hyperglycemia with increased fat metabolism and decreased protein synthesis occur ( Our body being exposed to this type of environment over years causes the development of many chronic conditions that would not have occurred if DM never took place in the body, all due to high glucose levels starting with not being properly displaced in the body as it should be normally.).
People with normal metabolism upon awaking and before breakfast are able to maintain blood glucose levels in the AM ranging from 60 to 110mg/dl. After eating food the non-diabetic’s blood glucose may rise to 120-140 mg/dl after eating (postprandial), but these then rapidly return back to normal. The reason for this happening is you eat food, it reaches the stomach, digestion takes place during digestion the stomach brakes down fats, carbohydrates, and sugars from compound sugars to simple sugars (fructose and glucose). Than the sugars transfer from the stomach into the bloodstream causing an increase in sugar levels. Now, your body uses the sugar it needs at that time throughout the entire body for energy and if still extra sugar left in the bloodstream that isn’t needed at that time to be utilized it now needs to go somewhere out of the bloodstream to allow the glucose blood level to get back between 60-110mg/dl. That extra glucose first gets stored up in the liver 60-80% and then gets stored in our fat tissue=fat storage=weight increase. Unfortunately this doesn’t take place with a diabetic since there is very little or no insulin being released by the pancreas and over time due to the high blood glucose blood levels (called hyperglycemia) problems arise in the body over years. When diabetes occurs there is a resolution and you have the disease the rest of your life. You need to control your glucose level.
Risk factors for Diabetes are either unmodified (factors we can’t control in out lives) OR modified=factors we can control in our lives (ex. diet, obese, habits (good or poor), and more.
2 TYPES OF DM: a.)Diabetes I & b.) Diabetes ll. We have risk factors that can cause disease/illness; there are unmodified and modified risk factors. With unmodified risk factors we have no control in them, which are 4 and these are: Heredity, Sex, Age, Race. Now modified risk factors are factors we can control, 3 of them that you can control is your weight, diet and health habits (which play a big role in why many people get diabetes II).
RISK FACTOR FOR TYPE DIABETES ONE:
Although the exact cause of type 1 diabetes is unknown, genetic factors can play a role. Your risk of developing type 1 diabetes increases if you have a parent or sibling who has type 1 diabetes. Based on research, we also know that genes account for less than half the risk of developing type1 disease. These findings suggest that there are other factors besides genes that influence the development of diabetes. We don’t know what these factors are, but a number of different theories exist. Environmental factors, such as exposure to a viral illness, also likely play some role in type 1 diabetes. Other factors that may increase your risk include:
The presence of damaging immune system cells that make autoantibodies. Sometimes family members of people with type 1 diabetes are tested for the presence of diabetes autoantibodies. If you have these autoantibodies, you have an increased risk of developing type 1 diabetes. But, not everyone who has these autoantibodies develops type 1.
Dietary factors.
-A number of dietary factors have been linked to an increased risk of type 1 diabetes, such as low vitamin D consumption; early exposure to cow’s milk or cow’s milk formula; or exposure to cereals before 4 months of age.
-Race. Type 1 diabetes is more common in whites than in other races.
-Geography.
-Certain countries, such as Finland and Sweden, have higher rates of type 1 diabetes.
RISK FACTORS FOR DIABETES TYPE 2 AND PREDIABETES
1-Researchers don’t fully understand why some people develop prediabetes and type 2 diabetes and others don’t. It’s clear that certain factors increase the risk, however, including:
2-Weight.
The more fatty tissue you have, the more resistant your cells become to insulin.
3-Inactivity.
The less active you are, the greater your risk. Physical activity helps you control your weight, uses up glucose as energy and makes your cells more sensitive to insulin. Exercising less than three times a week may increase your risk of type 2 diabetes.
4-Family history.
Your risk increases if a parent or sibling has type 2 diabetes.
5-Race.
Although it’s unclear why, people of certain races — including blacks, Hispanics, American Indians and Asians — are at higher risk.
6-Age.
Your risk increases as you get older. This may be because you tend to exercise less, lose muscle mass and gain weight as you age. But type 2 diabetes is also increasing dramatically among children, adolescents and younger adults.
7-Gestational Diabetes
If you developed gestational diabetes when you were pregnant, your risk of developing prediabetes and type 2 diabetes later increases. If you gave birth to a baby weighing more than 9 pounds (4 kilograms), you’re also at risk of type 2 diabetes.
8-Polycystic ovary syndrome.
For women, having polycystic ovary syndrome — a common condition characterized by irregular menstrual periods, excess hair growth and obesity — increases the risk of diabetes.
9-High blood pressure.
Having blood pressure over 140/90mm Hg is linked to an increased risk of type 2 diabetes.
10-Abnormal cholesterol levels.
If you have low levels of high-density lipoprotein (HDL), or “good,” cholesterol, your risk of type 2 diabetes is higher. Low levels of HDL are defined as below 35 mg/dL.
High levelsn of triglycerides. Triglycerides are a fat carried in the blood. If your triglyceride levels are above 250 mg/dL, your risk of diabetes increases.
RISK FACTORS FOR GESTATIONAL DIABETES (DIABETES 2):
1-Age.
1-Women older than age 25 are at increased risk.
3-Family or personal history.
4-Your risk increases if you have prediabetes — a precursor to type 2 diabetes — or if a close family member, such as a parent or sibling, has type 2 diabetes. You’re also at greater risk if you had gestational diabetes during a previous pregnancy, if you delivered a very large baby or if you had an unexplained stillbirth.
5-Weight.
Being overweight before pregnancy increases your risk.
6-Race.
7-For reasons that aren’t clear, women who are black, Hispanic, American Indian or Asian are more likely to develop gestational diabetes.
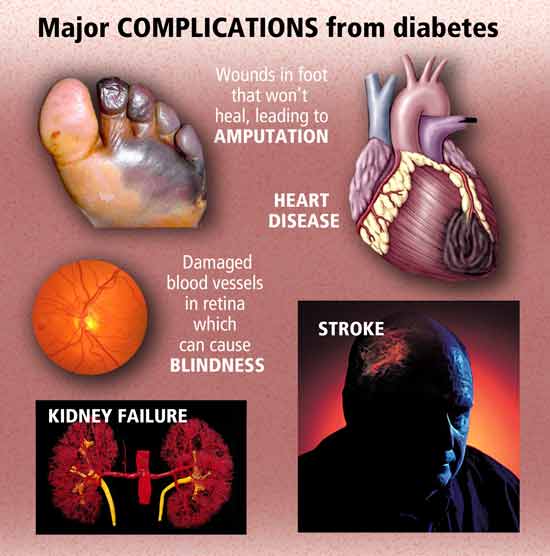
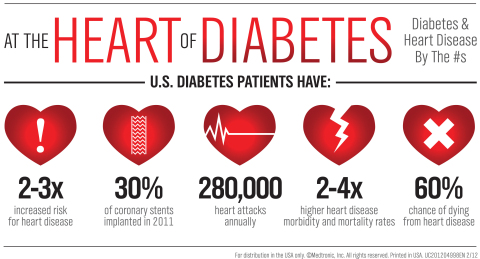
The key not to get diabetes is taking Prevention Measures (especially regarding type II) but even diagnosed with diabetes there are measures you can take in helping to control the glucose and decreasing the chances of increasing the side effects of what it can cause to the human body organs overtime especially cardiac disease, kidney disease, neuropathy, retinopathy to blind from having hyperglycemia frequently over years; in time it thickens the blood making circulation difficulty effecting tissues furthest from the heart= feet/lower extremities where skin ulcers occur for not getting enough oxygen to the tissues in the feet or lower extremities that can lead to necrosis causing amputation of toes to foot to below knee amputation to even above knee amputation. It also increases chance of heart attack and stroke.
PREVENTION first and CONTROL second when diagnosed with DM, is so vitally important.
So help control your diabetes through your diet (eating a low glucose or sugar diet=1800 to 2000 calories a day or as your m.d. prescribes for you), controlling your weight (get in therapeutic weight range), and practice healthy habits.