Know the symptoms of breast cancer are:
CDC says this:
“Different people have different symptoms of breast cancer. Some people do not have any signs or symptoms at all.
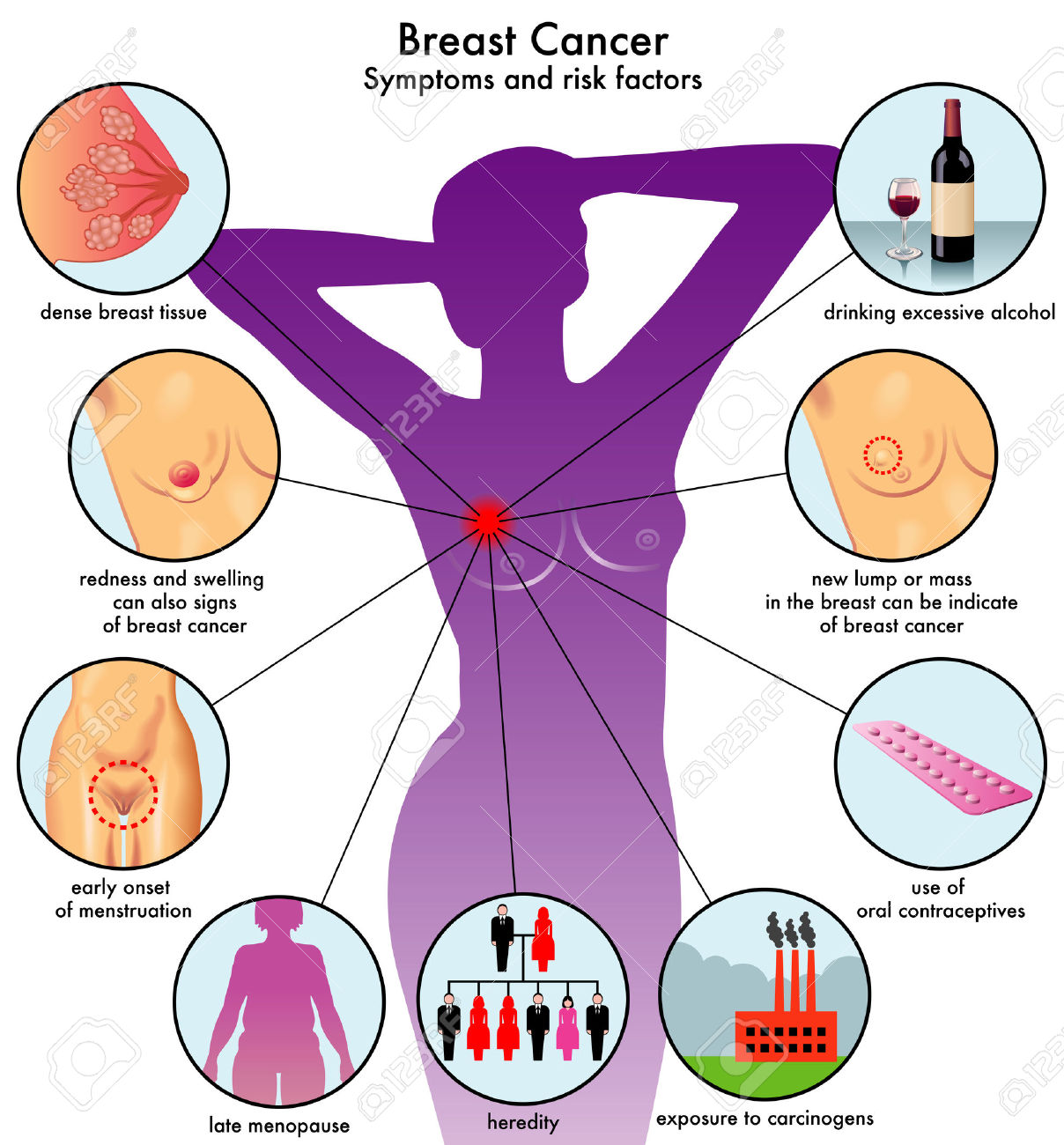
Some warning signs of breast cancer are—
- New lump in the breast or underarm (armpit).
- Thickening or swelling of part of the breast.
- Irritation or dimpling of breast skin.
- Redness or flaky skin in the nipple area or the breast.
- Pulling in of the nipple or pain in the nipple area.
- Nipple discharge other than breast milk, including blood.
- Any change in the size or the shape of the breast.
- Pain in any area of the breast.”
Is there a link between birth control pills and breast cancer?
A number of older studies suggested that birth control pills slightly increased the risk of breast cancer, especially among younger women. In these studies, however, 10 years after discontinuing birth control pills women’s risk of breast cancer returned to the same level as that of women who never used oral contraceptives. Current evidence does not support an increase in breast cancer with birth control pills.
Be vigilant about breast cancer detection. If you notice any changes in your breasts, such as a new lump or skin changes, consult your doctor. Also, ask your doctor when to begin mammograms and other screenings.
Once you’ve been diagnosed with breast cancer, your doctor works to find out the specifics of your tumor. Using a tissue sample from your breast biopsy or using your tumor if you’ve already undergone surgery, your medical team determines your breast cancer type. This information helps your doctor decide which treatment options are most appropriate for you. The biopsy helps what’s used to determine your breast cancer type.
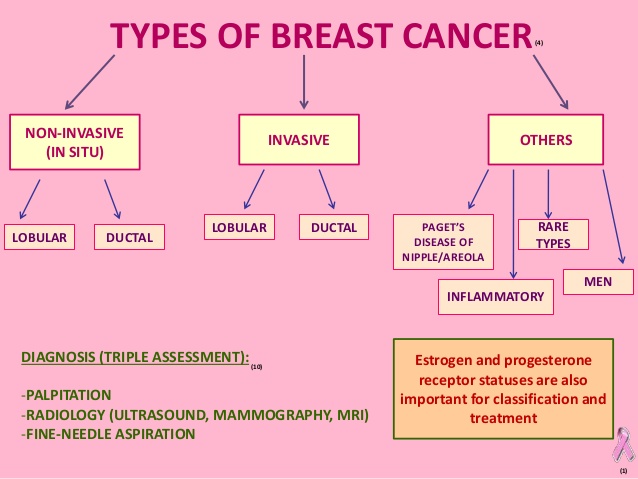
Is your cancer invasive or noninvasive?
Whether your cancer is invasive or noninvasive helps your doctor determine whether your cancer may have spread beyond your breast, which treatments are more appropriate for you, and your risk of developing cancer in the same breast or your other breast.
- Noninvasive (in situ) breast cancer. In situ breast cancer refers to cancer in which the cells have remained within their place of origin — they haven’t spread to breast tissue around the duct or lobule. One type of noninvasive cancer called ductal carcinoma in situ (DCIS) is considered a precancerous lesion. This means that if it were left in the body, DCIS could eventually develop into an invasive cancer. Another type of noninvasive cancer called lobular carcinoma in situ (LCIS) isn’t considered precancerous because it won’t eventually evolve into invasive cancer. LCIS does, however, increase the risk of cancer in both breasts.
- Invasive breast cancer. Invasive (infiltrating) breast cancers spread outside the membrane that lines a duct or lobule, invading the surrounding tissues. The cancer cells can then travel to other parts of your body, such as the lymph nodes. If your breast cancer is stage I, II, III or IV, you have invasive breast cancer.
In what part of the breast did your cancer begin?
The type of tissue where your breast cancer arises determines how the cancer behaves and what treatments are most effective. Parts of the breast where cancer begins include:
- Milk ducts. Ductal carcinoma is the most common type of breast cancer. This type of cancer forms in the lining of a milk duct within your breast. The ducts carry breast milk from the lobules, where it’s made, to the nipple.
- Milk-producing lobules. Lobular carcinoma starts in the lobules of the breast, where breast milk is produced. The lobules are connected to the ducts, which carry breast milk to the nipple.
- Connective tissues. Rarely breast cancer can begin in the connective tissue that’s made up of muscles, fat and blood vessels. Cancer that begins in the connective tissue is called sarcoma. Examples of sarcomas that can occur in the breast include phyllodes tumor and angiosarcoma.
FYI a complication that can occur with advanced cancer that many of you may be unaware of; bone metastasis.
Bone metastasis occurs when cancer cells spread from their original site to a location in the bone. The most common types of cancer more likely to spread to bone include breast, prostate and lung cancers.
Bone metastasis can occur in any bone, but more commonly occurs in the pelvis and spine. Bone metastasis may be the first sign that you have cancer, or it may occur years after your cancer treatment is completed, ex. Hodgkins Disease.
Signs and symptoms of bone metastasis may include the following:
- Bone pain (back and pelvic pain are most common)
- Unexplained broken bones
- Loss of urine and/or bowel function
- Weakness in the legs
- High levels of calcium in the blood (hypercalcemia), which can cause nausea, vomiting and confusion
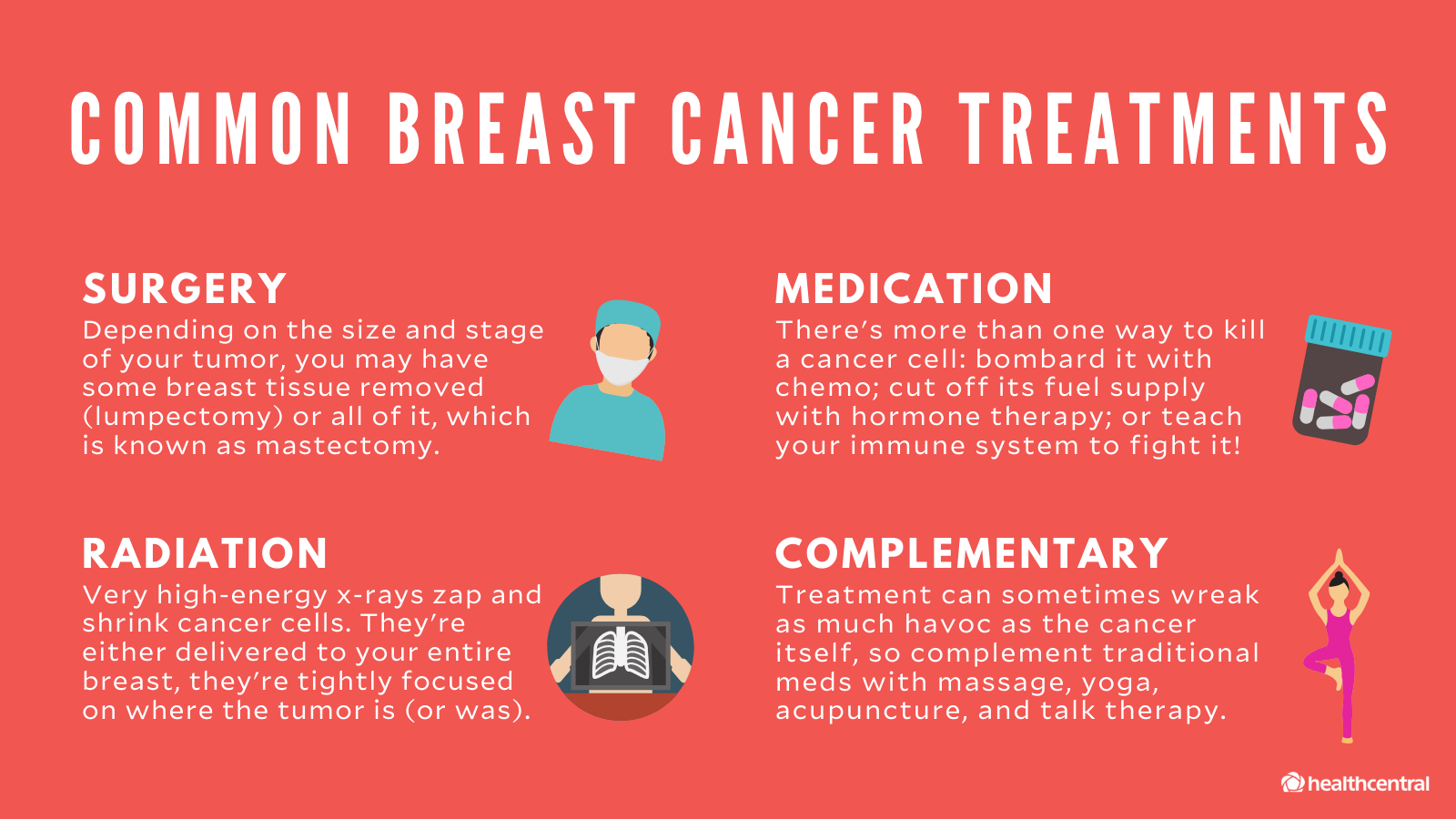
The most common problem with metastatic bone cancer is pain and fractures. Metastatic bone cancer usually can’t be cured, but instead the goal is to provide pain relief and control further spread. Treatment can make a big difference and may include the following:
- Medications to repair and build new bone — These medications are similar to those used by people with osteoporosis and can help in building and strengthening your bone.
- Chemotherapy — Given as a pill or through a vein, used to control and treat cancer that has spread to the bone.
- Traditional radiation therapy — Radiation is given as external beam therapy to treat the cancer in the bone.
- Hormone therapy — Medications are used to block hormones (for breast and prostate cancers) that help control the spread of cancer to the bone.
- Surgery — Used to fix a fracture and stabilize a break from the cancer in the bone.
- Cryoablation — A special technique that freezes the cancer cells.
- Radiofrequency ablation — A special technique that heats the cancer cells.
- Chemoradiation — A form of internal radiation that is given through the vein and travels to the site of bone metastasis and targets the cancer cells.
- Pain medications — Medications provided with the goal of relieving and controlling pain from bone metastasis.
- Physical therapy — Exercises may be prescribed to assist in strengthening muscles and providing any assistive devices that may help you (cane, walker, crutches, etc.).
If you’re living with metastatic bone cancer, you may find help and resources from a website called Bone Health in Focus. It was established with partners including BreastCancer.org, the National Lung Cancer Partnership and Us TOO International Prostate Cancer Education & Support Network to offer resources that help patients and caregivers understand more about cancer that has spread to the bone (find the site at www.bonehealthinfocus.com).
Mayo Clinic information on cancer that has spread to the bone can be found at http://www.mayoclinic.org/diseases-conditions/bone-metastasis/basics/definition/con-20035450.
Are you living with cancer that has spread to the bone? Feel free to share your experiences with each other on the this blog striveforgoodhealth.com or on TheMayoclinic.org.
Make the changes in your lifestyles including diet if you want to prevent cancer, live long and have a productive life.
REFERENCE: Mayoclinic.org
Article reviewed 10/18/2022