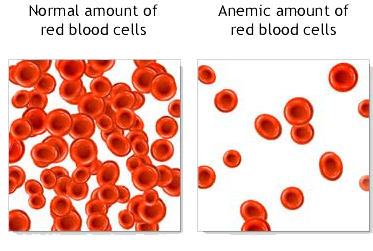
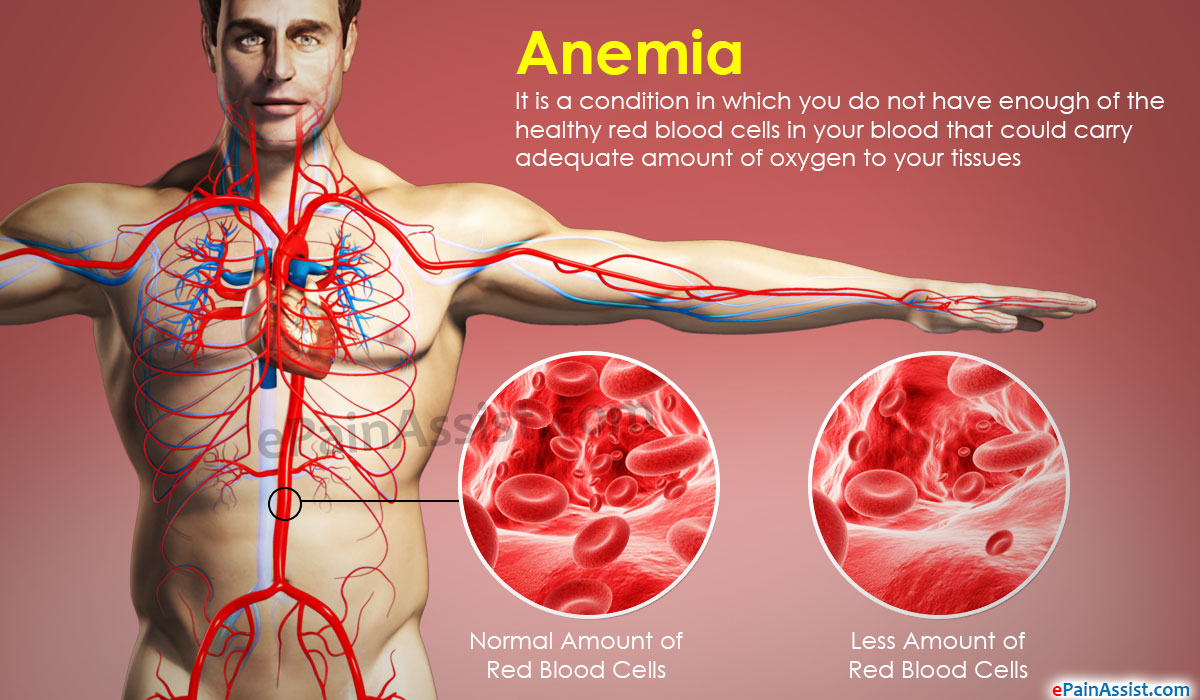
Anemia develops when you don’t have enough robust, healthy red blood cells to carry oxygen throughout your body. The blood cells may lack enough hemoglobin, the protein that gives blood its red color. Anemia affects one in 10 teen girls and women. It also develops in men and children and is linked to some illnesses. Anemia is a condition that develops when your blood lacks enough healthy red blood cells or hemoglobin. Hemoglobin is a main part of red blood cells and binds oxygen. If you have too few or abnormal red blood cells, or your hemoglobin is abnormal or low, the cells in your body will not get enough oxygen. Symptoms of anemia — like fatigue — occur because organs aren’t getting what they need to function properly.
Anemia is the most common blood condition in the U.S. It affects about 3.5 million Americans. Women, young children, and people with chronic diseases are at increased risk of anemia.
There types of different anemia’s but today’s we’ll look more into is Iron Deficiency Anemia.
Iron deficiency anemia is a common type of anemia — a condition in which blood lacks adequate healthy red blood cells. Red blood cells carry oxygen to the body’s tissues.
As the name implies, iron deficiency anemia is due to insufficient iron. Without enough iron, your body can’t produce enough of a substance in red blood cells that enables them to carry oxygen (hemoglobin). As a result, iron deficiency anemia may leave you tired and short of breath.
You can usually correct iron deficiency anemia with iron supplementation. Sometimes additional tests or treatments for iron deficiency anemia are necessary, especially if your doctor suspects that you’re bleeding internally.
Initially, iron deficiency anemia can be so mild that it goes unnoticed. But as the body becomes more deficient in iron and anemia worsens, the signs and symptoms intensify.
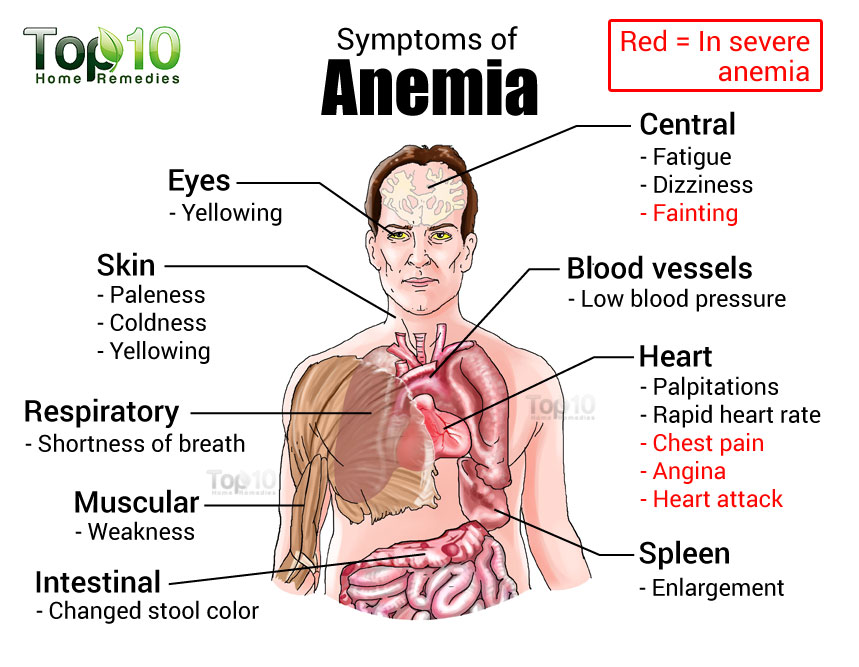
Iron deficiency anemia symptoms may include:
- Extreme fatigue, Pale skin, Weakness, Shortness of breath, Chest pain, Frequent infections
- Headache, Dizziness or lightheadedness, Cold hands and feet, Inflammation or soreness of your tongue, Brittle nails, and Fast heartbeat.
- Unusual cravings for non-nutritive substances, such as ice, dirt or starch.
- Poor appetite, especially in infants and children with iron deficiency anemia.
- An uncomfortable tingling or crawling feeling in your legs (restless legs syndrome).
Causes of iron deficiency anemia include:
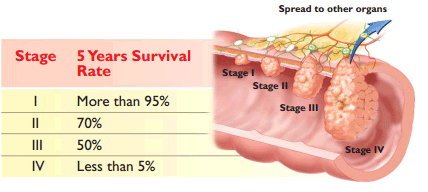
- Blood loss. Blood contains iron within red blood cells. So if you lose blood, you lose some iron. Women with heavy periods are at risk of iron deficiency anemia because they lose blood during menstruation. Slow, chronic blood loss within the body — such as from a peptic ulcer, a hiatal hernia, a colon polyp or colorectal cancer — can cause iron deficiency anemia. Gastrointestinal bleeding can result from regular use of some over-the-counter pain relievers, especially aspirin.
- A lack of iron in your diet. Your body regularly gets iron from the foods you eat. If you consume too little iron, over time your body can become iron deficient. Examples of iron-rich foods include meat, eggs, leafy green vegetables and iron-fortified foods. For proper growth and development, infants and children need iron from their diet, too.
- An inability to absorb iron. Iron from food is absorbed into your bloodstream in your small intestine. An intestinal disorder, such as celiac disease, which affects your intestine’s ability to absorb nutrients from digested food, can lead to iron deficiency anemia. If part of your small intestine has been bypassed or removed surgically, that may affect your ability to absorb iron and other nutrients.
- Without iron supplementation, iron deficiency anemia occurs in many pregnant women because their iron stores need to serve their own increased blood volume as well as be a source of hemoglobin for the growing fetus.
Those at risk for anemia:
Anemia is a common condition. It occurs in all age, racial, and ethnic groups. Both men and women can have anemia. However, women of childbearing age are at higher risk for the condition because of blood loss from menstruation.
Anemia can develop during pregnancy due to low levels of iron and folic acid (folate) and changes in the blood. During the first 6 months of pregnancy, the fluid portion of a woman’s blood (the plasma) increases faster than the number of red blood cells. This dilutes the blood and can lead to anemia.
During the first year of life, some babies are at risk for anemia because of iron deficiency. At-risk infants include those who are born too early and infants who are fed breast milk only or formula that isn’t fortified with iron. These infants can develop iron deficiency by 6 months of age.
Infants between 1 and 2 years of age also are at risk for anemia. They may not get enough iron in their diets, especially if they drink a lot of cow’s milk. Cow’s milk is low in the iron needed for growth.
Drinking too much cow’s milk may keep an infant or toddler from eating enough iron-rich foods or absorbing enough iron from foods.
Older adults also are at increased risk for anemia. Researchers continue to study how the condition affects older adults. Many of these people have other medical conditions as well.
Major Risk Factors for anemia:
- A diet that is low in iron, vitamins, or minerals
- Blood loss from surgery or an injury
- Long-term or serious illnesses, such as kidney disease, cancer, diabetes, rheumatoid arthritis, HIV/AIDS, inflammatory bowel disease (including Crohn’s disease), liver disease, heart failure, and thyroid disease
- Long-term infections
- A family history of inherited anemia, such as sickle cell anemia or thalassemia.
Complications of Anemia:
Some people who have anemia may have arrhythmias. Arrhythmias are problems with the rate or rhythm of the heartbeat. Over time, arrhythmias can damage your heart and possibly lead to heart failure.
Anemia also can damage other organs in your body because your blood can’t get enough oxygen to them.
Anemia can weaken people who have cancer or HIV/AIDS. This can make their treatments not work as well.
Anemia also can cause many other health problems. People who have kidney disease and anemia are more likely to have heart problems. With some types of anemia, too little fluid intake or too much loss of fluid in the blood and body can occur. Severe loss of fluid can be life threatening.