Middle East respiratory syndrome (MERS) is a viral respiratory illness caused by a coronavirus (Middle East respiratory syndrome coronavirus, or MERS‐CoV) that was first identified in Saudi Arabia in 2012.
Coronaviruses are a large family of viruses that can cause diseases in humans, ranging from the common cold to Severe Acute Respiratory Syndrome (SARS).
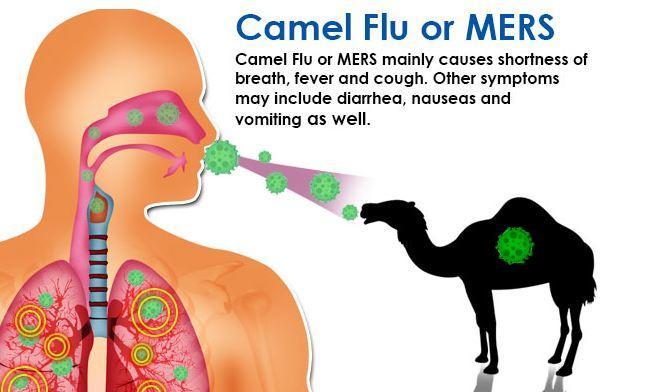
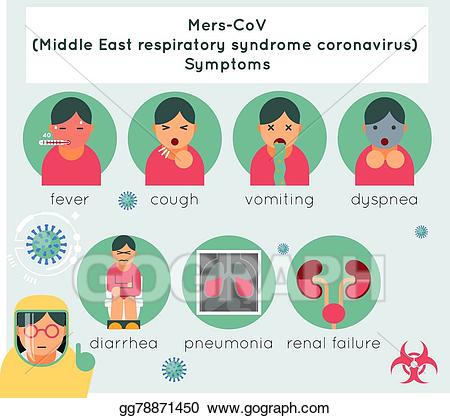
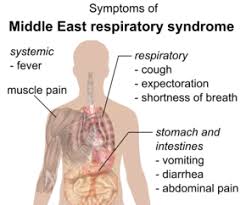
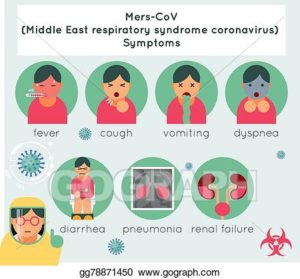
A typical case of MERS includes fever, cough, and/or shortness of breath. Pneumonia is common, however some people infected with the MERS virus have been reported to be asymptomatic. Gastrointestinal symptoms, including diarrhoea, have also been reported.
Severe cases of MERS can include respiratory failure that requires mechanical ventilation and support in an intensive-care unit.
Some patients have had organ failure, especially of the kidneys, or septic shock. The virus appears to cause more severe disease in people with weakened immune systems, older people, and people with chronic diseases as diabetes, cancer, and chronic lung disease.
The mortality rate for people with the MERS virus is approximately 35% – this may be an overestimate however, as mild cases may be missed by existing surveillance systems.
Infected people with no symptoms have been identified because they were tested for MERS-CoV during investigations among contacts of people known to be infected with MERS-CoV. The role of asymptomatic infected individuals in transmission is currently unknown and under investigation.
It is not always possible to identify people infected with the MERS virus because early symptoms of the disease are non-specific.
MERS has been reported in 27 countries since 2012, with approximately 80% of human cases reported by the Kingdom of Saudi Arabia.
Cases identified outside the Middle East are people who were infected in the Middle East and travelled to areas outside the Middle East. On rare occasions, small outbreaks have occurred in areas outside the Middle East.
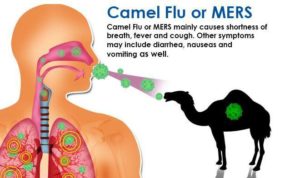
The MERS virus is transmitted primarily from infected dromedary camels to people, but transmission from people to people is also possible.
From animals to people
MERS-CoV is a zoonotic virus, meaning it is transmitted between animals and people. Scientific evidence suggests that people are infected through unprotected direct or indirect contact with infected dromedary camels.
The MERS virus has been identified in dromedary camels in several countries, including Burkina Faso, Egypt, Ethiopia, Iran, Jordan, Kenya, Kingdom of Saudi Arabia, Kuwait, Mali, Morocco, Netherlands, Nigeria, Oman, Pakistan, Qatar, Spain (Canary Islands), Somalia, Sudan, Tunisia, and the United Arab Emirates.. There is further evidence suggesting the MERS-CoV is widespread in dromedary camels in the Middle East, Africa and South Asia.
The dromedary, also called the Arabian camel (Camelus dromedarius), is a large, even-toed ungulate with one hump on its back. It is the tallest of the three species of camel; adult males stand 1.8–2 m (5.9–6.6 ft) at the shoulder, while females are 1.7–1.9 m (5.6–6.2 ft) tall. Males typically weigh between 400 and 600 kg (880 and 1,320 lb), and females weigh between 300 and 540 kg (660 and 1,190 lb). The species’ distinctive features include its long, curved neck, narrow chest, a single hump (compared with two on the Bactrian camel and wild Bactrian camel), and long hairs on the throat, shoulders and hump. The coat is generally a shade of brown. The hump, 20 cm (7.9 in) tall or more, is made of fat bound together by fibrous tissue.
Dromedaries are mainly active during daylight hours. They form herds of about 20 individuals, which are led by a dominant male. This camel feeds on foliage and desert vegetation; several adaptations, such as the ability to tolerate losing more than 30% of its total water content, allow it to thrive in its desert habitat. Mating occurs annually and peaks in the rainy season; females bear a single calf after a gestation of 15 months.
The dromedary has not occurred naturally in the wild for nearly 2,000 years. It was probably first domesticated in Somalia or the Arabian Peninsula about 4,000 years ago. In the wild, the dromedary inhabited arid regions, including the Sahara Desert. The domesticated dromedary is generally found in the semi-arid to arid regions of the Old World, mainly in Africa, and a significant feral population occurs in Australia. Products of the dromedary, including its meat and milk, support several north Arabian tribes; it is also commonly used for riding and as a beast of burden (people riding the camel for work).
This is how this illness got the nick name “Camel Flu”, based on the geographical area it initially came from, being the Middle East.
It is possible that other animal reservoirs exist, however animals including goats, cows, sheep, water buffalo, swine, and wild birds have been tested for MERS-CoV and the virus has not been found.
Between people
The MERS virus does not pass easily between people unless there is close unprotected contact, such as the provision of clinical care to an infected patient without strict hygiene measures.
Transmission between people has been limited to-date, and has been identified among family members, patients, and health care workers. The majority of reported MERS cases to date have occurred in health care settings.
If you have had close contact with someone infected with MERS-CoV within the last 14 days without using the recommended infection control precautions, you should contact a healthcare provider for an evaluation.
As a general precaution, anyone visiting farms, markets, barns, or other places where animals are present should practice general hygiene measures. These include regular hand-washing before and after touching animals, and avoiding contact with sick animals.
The consumption of raw or undercooked animal products, including milk and meat, carries a high risk of infection from a variety of organisms. Animal products processed appropriately through cooking or pasteurization are safe for consumption, but should also be handled with care to avoid cross-contamination with uncooked foods. Camel meat and camel milk are nutritious products that can be consumed after pasteurization, cooking, or other heat treatments.
Until more is understood about MERS-CoV, people with diabetes, renal failure, chronic lung disease, and immunocompromised persons are considered to be at high risk of severe disease from MERS-CoV infection. Especially in the Middle East, this group of people should avoid contact with dromedary camels, consuming raw camel milk or camel urine, as well as eating meat that has not been properly cooked.
Health care workers are at risk for transmission of MERS-CoV, it has occurred in health care facilities in several countries, most notably in Saudi Arabia and the Republic of Korea.
Droplet precautions should be added to standard precautions when providing care to all patients with symptoms of acute respiratory infection. Contact precautions and eye protection should be added when caring for suspected or confirmed cases of MERS. Airborne precautions should be applied when performing aerosol‐generating procedures.
SARS is the other major concern if a patient is diagnosed with COVID-19. Both MERS and/or SARS can lead to death especially in the elderly.