Complications of Cushings Syndrome include:
Diabetes (High or Low blood glucose levels)
Enlargement of pituitary tumor and other complications from the tumor growth
Fractures due to osteoporosis which are common in older people
High blood pressure which could be life threatening
Kidney stones from the increase in cortisol and other chemicals filtered through the kidneys
Serious infections which could lead to further secondary infections
Although diagnosis can be challenging, it is important being correctly diagnosed with Cushing’s disease is the first step toward regaining control of your health because an accurate diagnosis helps your doctor determine the best course of action. Cushing’s disease may be challenging to diagnose because of several factors:
Cushing’s disease does not cause the same symptoms in everyone
Cushing’s disease may cause the same symptoms as other medical conditions that are more common
The tumor that causes Cushing’s disease can be too small to be found on MRI scans
The tumor can become “inactive” so that it releases less cortisol at certain times
Inactive tumors can fool tests for Cushing’s disease that measure the levels of hormones in your urine, blood, or saliva
The process and tests used to diagnose Cushing’s disease
Ways to take control of your health once you are diagnosed
Cushing’s disease can be mistaken for other conditions
Doctors don’t always think to look for Cushing’s disease because it is rare and causes symptoms that can make them think you have a different condition. Because these other conditions are more common, your doctor will probably rule them out before testing you for Cushing’s disease. These conditions include:
-Pregnancy
-Depression or other psychiatric disorders
-Alcoholism
-Weight problems (obesity) caused by improper diet and/or exercise
-Poorly controlled diabetes mellitus
-Polycystic ovarian syndrome (PCOS)
How is Cushing’s syndrome diagnosed?
The process of diagnosing Cushing’s disease—There are generally 3 phases in the diagnostic process and you will likely see more than one doctor, including an endocrinologist.
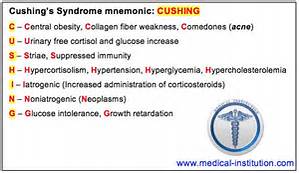
Phase 1: Confirm clinical suspicion-Your doctor will to a physical exam.
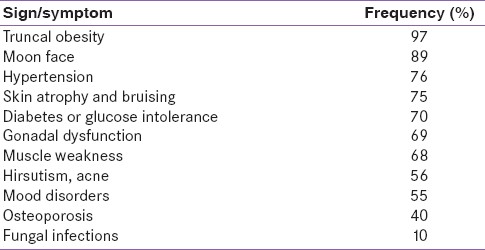
The doctor will measure if you have the symptoms that are known to be caused by hypercortisolism.
Your doctor may look for:
Purplish streaks on your body (called striae)
Weight gain
Fatty tissue around your mid-section
Thinning of your arms and legs
Fatty tissue that creates a hump on your back
Redness or roundness in your face
Bruises on your body
Thinning of your skin
Excessive facial/hair growth (hirtusism) if you’re female
Acne
Weakness
Medical conditions that are unusual for a patient’s age
— High blood pressure (called hypertension)
— Diabetes
— High cholesterol
— Osteoporosis
— Infection
— Heart disease
__Evaluation
What you can expect is your doctor will do a physical examine your entire body to look for specific physical signs of Cushing’s disease and may do tests to better understand your symptoms, what we call diagnostic tooling.
Phase II: Confirm hypercortisolism
Medical tests will be performed to measure the level of cortisol in the body. These tests should only be done when a form of Cushing’s syndrome(including Cushing’s disease) is highly suspected.
-24 hour urinary free cortisol (UFC) –
Measures the level of cortisol in your urine over a 24-hour period. If the levels are too high, then you may have Cushing’s disease or Cushing’s syndrome. This test is often used because it only measures the type of cortisol that causes Cushing’s disease, called “circulating cortisol,” and may be more accurate than other tests that measure cortisol levels
Because of the difficulty in obtaining 24-hour urine collections in many outpatients, some physicians use a l-mg overnight dexamethasone suppression test. For this test, the patient takes l mg of dexamethasone orally at 11 p.m., and the plasma cortisol level is measured at 8 a.m. the following day (normal value: 5 μg per dL or less [140 nmol per L]). The reported sensitivity of this test is 98 percent; the reported specificity is 80 percent.4
Obesity, chronic illness, chronic alcoholism and depression can cause false-positive results (pseudo-Cushing’s syndrome) on the 1-mg dexamethasone suppression test and mildly elevated free cortisol values on the 24-hour urine collection.
If the result of the dexamethasone suppression test is abnormal or the 24-hour urinary free cortisol level is mildly elevated, a confirmatory test for Cushing’s syndrome is needed. The 24-hour urine collection for urinary free cortisol excretion can be used to confirm the result of the l-mg dexamethasone suppression test. Normal findings on both tests provide strong evidence against the presence of Cushing’s syndrome.4 However, when Cushing’s syndrome is still strongly suspected based on the clinical findings, negative tests should be repeated; the tests should also be performed again in three to six months.
Phase III: Determine if Cushing’s disease is the cause of hypercortisolism
-Adrenocorticotropic Hormone (ACTH) test-
Measures if the amount of ACTH in your blood is higher than normal.
If your ACTH levels are high or normal, then you may have a tumor that is producing ACTH.
ACTH-producing tumors are most often found on the pituitary (Cushing’s disease).
ACTH-producing tumors may be in other areas of the body (called ectopic Cushing’s syndrome) If your ACTH levels are low, you may have Cushing’s syndrome due to a different cause or another condition. Additional tests will be done to confirm whether or not you have Cushing’s syndrome
Treatment of cushings syndrome is by castigation of the under lying cause.
Treatments for Cushing’s syndrome are contrived to pass your body’s cortisol production to normal. By indurate, or even distinctly lowering cortisol levels, you’ll feel evident improvements in your signs and symptoms. Left untreated, however, Cushing’s syndrome can finally induce to death. The treatment choice depend on the cause. For example:
-If a tumour in an adrenal gland is the reason, an operation to withdraw it will cure the condition.
– For adrenal hyperplasia, both adrenal glands may require to be withdraw. You will then require to take lifelong replacement therapy of several adrenal hormones.
-Other tumours in the body that produce ‘ectopic’ ACTH may be able to be removed, depending on the kind of tumour, where it is, etc.
-Medication to block the production or consequence of cortisol may be an choice.