

 BEES
BEES

 WASPS
WASPSSpring with summer around the corner have certain insects coming out of hibernation which are little insects with STINGERS and know how to deal with them.
Yes it’s that time of the year again better weather and getting warmer with certain individual insects waking up and popping into our site again that go BUZZZZZZZZZZZZZZ. Enjoy the weather but know these insect stingers and what to do.
At least 40 deaths occur each year in the U.S. as a result of serious anaphylactic sting reactions.
In general there are over 20,000 known bee species in the world, and 4,000 of them are native to the United States. They range from the tiny (2 mm) and solitary Perdita minima, known as the world’s smallest bee, to kumquat-sized species of carpenter bees. Our bees come in as many sizes, shapes, and colors as the flowers they pollinate. There is still much that we don’t know about native bees—many are smaller than a grain of rice and about 10% of bees in the United States have yet to be named or described—but all of these bees have jobs as pollinators.
A bee sting is strictly a sting from a bee (honey bee, bumblebee, sweat bee, etc.).
In the vernacular it can mean a sting of a bee, or even a wasp, or a hornet, or or a yellow jacket. Some people may even call the bite of a horse-fly a bee sting. The stings of most of these species can be quite painful, and are therefore keenly avoided by many people.
Honey bee stings release pheromones that prompt other nearby bees to attack.
Bee stings differ from insect bites, and the venom or toxin of stinging insects is quite different. Therefore, the body’s reaction to a bee sting may differ significantly from one species to another.
In people with insect sting allergy, a bee sting may trigger a local reaction meaning its at the site where you were stung which is redness, swelling, pain, and oozing possibly but a systemic reaction which can be dangerous meaning a anaphylactic reaction that is potentially deadly.
In general there are over 25,000 species of wasps found throughout the world. Some of the most common wasps include:
The yellow jacket and hornet, both of which live in groups, or colonies, in temperate climates.
Yellow jackets, which have black and yellow stripes on the abdomen, form underground nests.
Hornets are predominantly black with some yellow markings on the head and thorax. Hornets form paper-like nests that are attached to trees, bushes, or buildings.
Certain animals have developed stinging as a form of defense or hunting. Venomous stings can have a local reaction, meaning pain, swelling, redness, itching, and possible oozing around the sting site, or a systemic reaction, meaning with local symptoms plus hives or airway and circulatory problems across the whole body. Local symptoms meaning the reaction to the sting is in one local area and systemic meaning the reaction is generalized throughout the body.
Types of Wasps:
A-Hornets
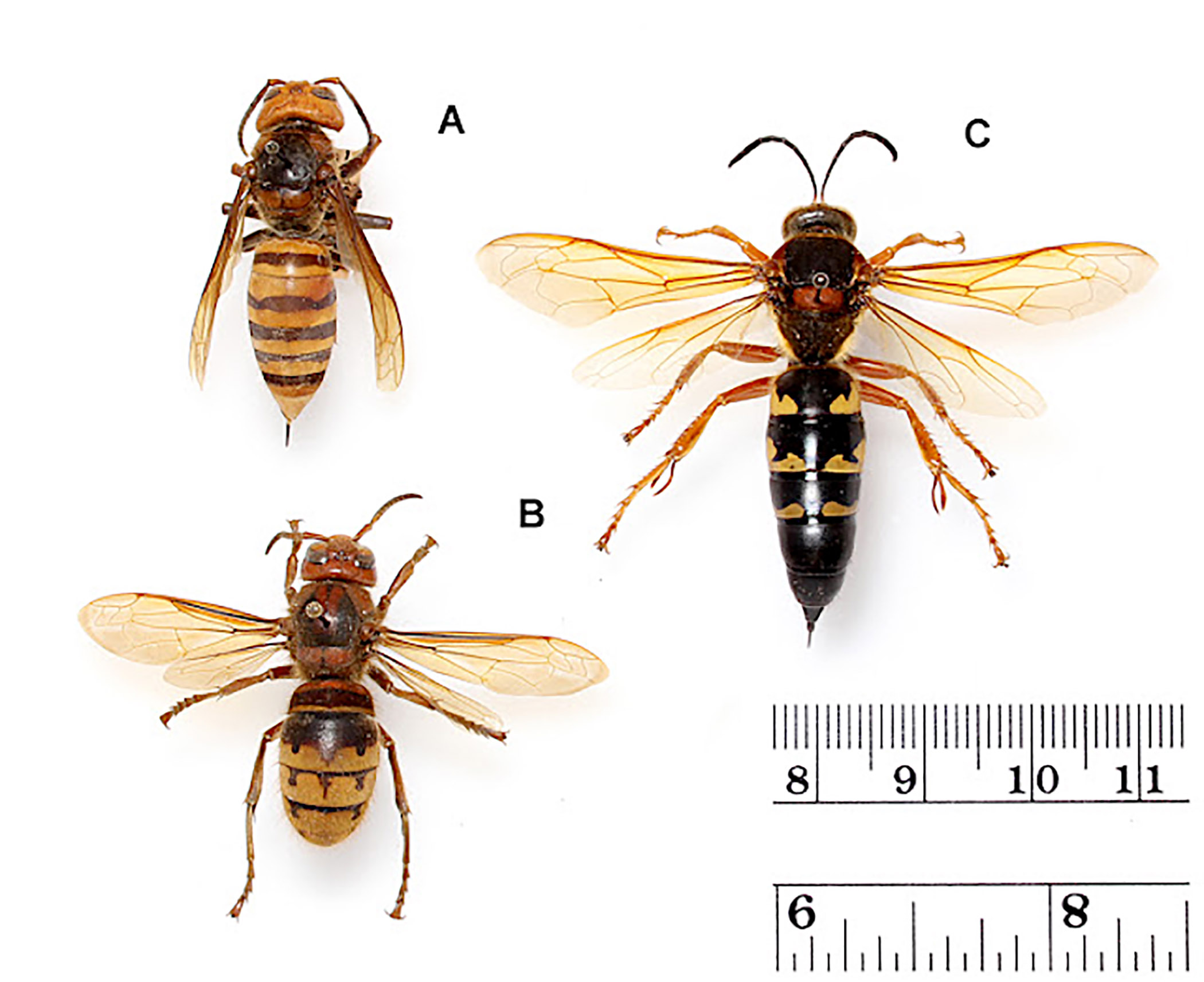
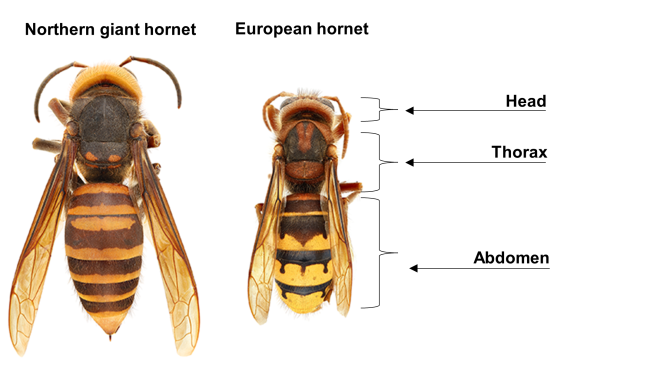
Hornets are a type of wasp closely related to and resembling yellow jackets, according to National Geographic. While the majority of the approximately 20 species of hornets are found in tropical parts of Asia, these stinging insects can also be found throughout Europe, Africa and North America. Hornets are social insects that live in community hives dominated by queens.They are considered pests and potentially dangerous by many because they aggressively defend their hives by using their stingers. Reacting quickly after disturbing a hornets’ nest will help you prevent excessive stings and potential allergic reactions.
Hornets are a large species of wasp, growing up to 2 1/2-inches in length. Hornets become aggressive when they feel threatened or must defend their nest. Unlike a bee, hornets can sting multiple times, as their stingers are not barbed. A hornet sting delivers venom beneath the skin that causes a painful reaction for up to three days following. You can treat a hornet sting to relieve some of the pain and swelling, making the healing process tolerable. Hornets are very, very painful. As soon as you are stung by a Hornet a red welt will develop and the throbbing pain will begin. Before trying to treat a Hornet sting be sure you are safely away from the Hornet and nest. A Hornet will sting many times and if you kill a Hornet their Hornet friends back at the nest will come after you too. When a Hornet is killed it releases a scent and other Hornets will come to investigate. If you are allergic to Hornet stings seek emergency medical attention 911 for anaphylactic reactions.
B.) Yellow Jackets 

Overall, stinging wasps have warning colors, either yellow, brown, to even blue or red. Wasps have pointed abdomens attached to the thorax by a thin waist called a petiole. They build papery nests from wood fibers, very common in the northeast. The colonies that live in these nests are led by one egg-laying queen. The female nest-building workers are the only ones with stingers, which are modified egg laying apparatuses. If threatened, they will gather into a stinging swarm to protect the nest.
C.) Solitary Wasps
There are two main types of wasps, the solitary ones and the social ones, which nest together. Here’s a quick look at each of these.
D.) Social Wasps 


For wasps, being social does not mean that they live in large colonies–far from it. A typical wasp nest can contain only a dozen individuals. The larger wasp nests can contain as many as 10,000 individuals, way below the 50,000 workers in a bee colony.
E.) Solitary Wasps
MALE  FEMALE
FEMALE 
In mid to late summer in the northeastern US, several species of large solitary wasp (belonging to the families Sphecidae and Crabronidae) frequent gardens, parks, and other open spaces. Despite their threatening appearance, solitary wasps are totally harmless. They are more interested in hunting other invertebrates–like spiders, flies, and bees–than they are in you. Solitary wasps are carnivores that capture and paralyze insects or spiders to feed their young, with many species specializing on particular types of prey. Unlike hornets, yellowjackets, and other social wasps, solitary wasp females build and provision nests independently of one another. Nesting locations differ among species and may include a variety of cavities both above and below ground.
The vast majority of wasps belong to the solitary type and they are mostly predators. Here are the main groups of solitary wasps:
- 1 Cuckoo wasps, which belong in the Chrysididae family
- 2 Tiphiid wasps of the Tiphiidae family
- 3 Scoliid wasps of the Scoliidae family
- 4 Velvet wasps of the family Mutillidae
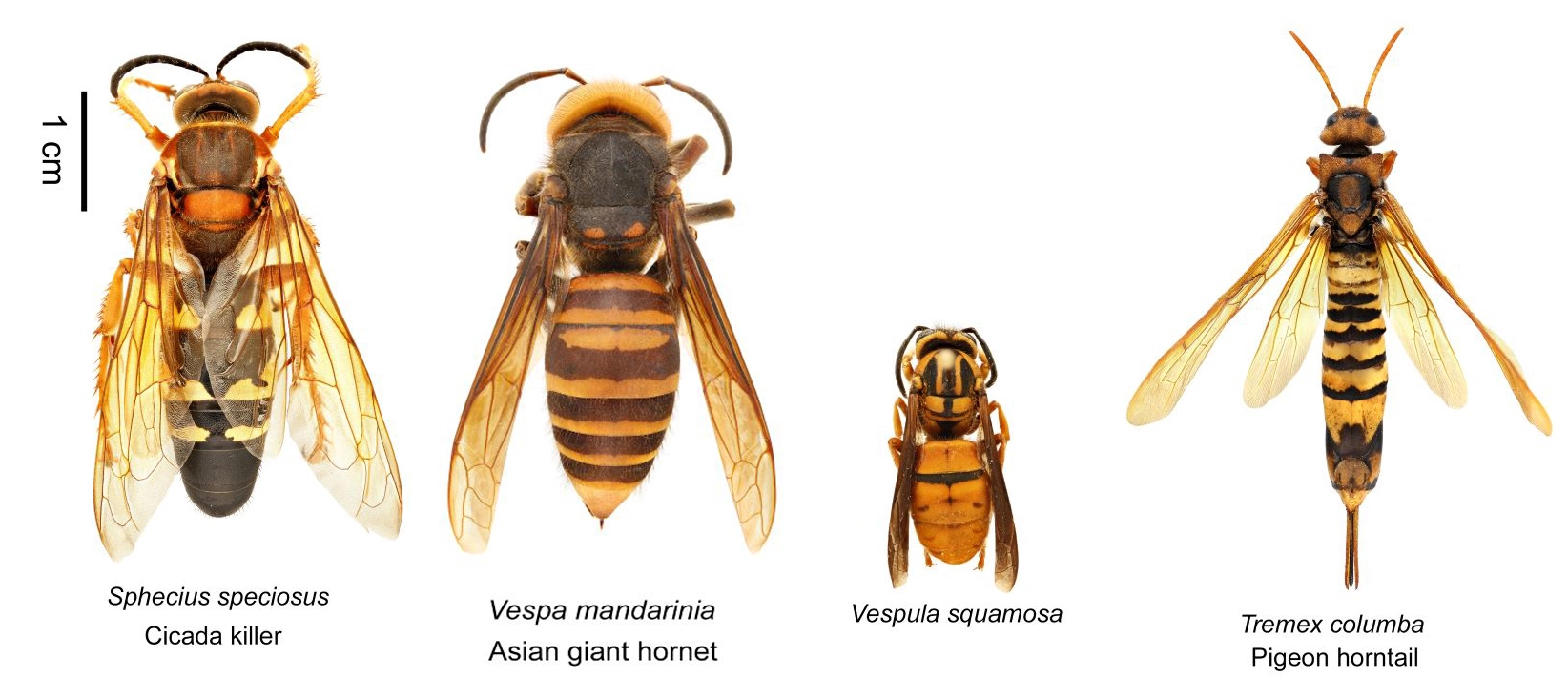
- 5 Cicada-killer
Solitary wasps are generally parasitic and do not build colonies, unlike their more social relatives.

#1 Cockoo Cockoo Wasp Digital photo of a female #1
#2 Tiphiid Wasps 

#3 Adult Scoliid Wasp of the Subfamily Campsomerinae


#5 Cicada Killer Wasp 

REMEMBER wasps have the ability to sting repeatedly.
Treat a wasp, hornet, or yellow jacket with care. If you get stung, leave the area and wash with soap and water as soon as you can. Applying a cold compress can help reduce swelling. Although if your symptoms worsen more than mild pain and swelling seek medical attention ASAP!
Tune into Part 2 tomorrow for learning about the BEES.