
Kawasaki disease (KD), also known as Kawasaki syndrome, is a severe illness characterized by inflammation of blood vessels throughout the body that primarily affects young children and infants. Kawasaki disease is the leading cause of acquired heart disease in children. Although about 80 percent of patients are under five years of age, older children and teenagers can also get KD, but this is uncommon. KD is more common in boys than girls, and the majority of cases are diagnosed in the winter and early spring. KD is not contagious.
The disease is named after Tomisaku Kawasaki, a Japanese pediatrician who first described the illness in the medical literature in 1967. Although it is more prevalent among children of Asian and Pacific Island descent, KD affects people of all racial and ethnic groups.
It is estimated that more than 4,200 children are diagnosed with Kawasaki Disease in the U.S. each year. The cause of KD is unknown, although an agent, like a virus, is suspected. There is no currently accepted scientific evidence that KD is caused by carpet cleaning or chemical exposure.
There is no specific test for KD; doctors make a clinical diagnosis based on a collection of symptoms and physical findings.
Symptoms
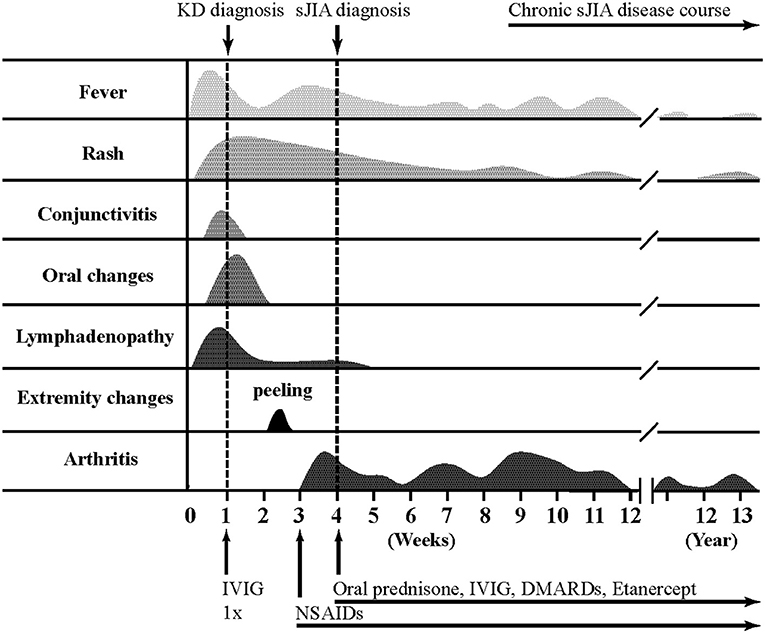
Kawasaki disease symptoms usually appear in three phases. Early symptoms of KD include:
Phase 1
- A fever that is often higher than 102.2 F (39 C) and lasts at least five days
- Bloodshot eyes (conjunctivitis) without a thick discharge
- A rash on the main part of the body (trunk) and/or in the genital area
- Red, dry, cracked lips and an extremely red, swollen tongue (strawberry tongue)
- Swollen, red skin on the palms of the hands and the soles of the feet
- Swollen lymph nodes in the neck
Phase 2
In the second phase of the disease, the symptoms may include:
- Peeling of the skin on the hands and feet, especially the tips of the fingers and toes
- Joint pain
- Diarrhea
- Vomiting
- Abdominal pain
Phase 3
In the third phase of the disease, signs and symptoms will slowly fade away unless complications develop. Patients experiencing Kawasaki disease may experience tiredness, irritability and low energy for as long as eight weeks post the initial diagnosis.
Treatment and Complications
To reduce the risk of coronary artery complications, treatment for KD shall be started within ten days of the onset of symptoms. Most KD patients will recover from KD without any lasting heart damage; however, without treatment, about 25% of KD patients will develop abnormalities of the coronary arteries. Treatment for KD may include:
- Gamma globulin (to lower the risk of coronary artery problems)
- Aspirin (to treat inflammation, decrease pain and joint inflammation, as well as reduce the fever)
Kawasaki treatment is a rare exception to the rule against aspirin use in children but only when given under the supervision of your child’s doctor. Children who develop coronary artery abnormalities may be required to continue taking aspirin for six weeks or longer to prevent clotting. Taking aspirin has been linked to Reye’s Syndrome, a rare but potentially life-threatening condition that can affect the blood, liver, and brain of children and teenagers after a viral infection. Children who develop chickenpox or the flu during aspirin treatment may be required to stop taking aspirin.