“It’s that time of year again and the list of presents to buy for family and friends may only seem longer.
Before stuffing your shopping bags – or online cart, more likely – doctors say parents should be aware of unassuming toys and accessories (for others in the family) that land babies and small children in the emergency room each year.
“We do see a spike during the holiday season,” said Dr. Robert Kramer, a pediatric gastroenterologist at Children’s Hospital Colorado. “But it’s something we have to be vigilant for at all times.”
In recent years, the U.S. Consumer Product Safety Commission (CPSC) has created a robust toy safety system, by requiring testing by independent, third party testing laboratories around the world; enforcing stringent lead and phthalatesPhthalates, or phthalate esters, are esters of phthalic anhydride. They are mainly used as plasticizers, i.e., substances added to plastics to increase their flexibility, transparency, durability, and longevity. They are used primarily to soften polyvinyl chloride. ( limits for toys; imposing some of the most stringent toy standards in the world; and stopping violative and dangerous toys at the ports and in the marketplace before they reach children’s hands). These combined efforts continue to foster the confidence of American families as they prepare to shop for toys this holiday season.
Safety tips to keep in mind this holiday season:
Balloons Children can choke or suffocate on deflated or broken balloons. Keep deflated balloons away from children younger than eight years old. Discard broken balloons immediately.
Small balls and other toys with small parts For children younger than age three, avoid toys with small parts, which can cause choking.
Scooters and other riding toys
Riding toys, skateboards and in-line skates go fast, and falls could be deadly. Helmets and safety gear should be worn properly at all times and they should be sized to fit.
Magnets
High-powered magnet sets are dangerous and should be kept away from children. Whether marketed for children or adults, building and play sets with small magnets should also be kept away from small children.
Button Batteries
Button batteries are typically about 20 millimeters in diameter, or between the size of a penny and a nickel, according to the National Capital Poison Center. They’re used in a wide variety of household items and products, including hearing aids, key fobs and children’s toys.
“The majority of the injuries from button batteries are going to be from swallowing them,” Martin explained, adding that the screws typically used to secure the batteries inside products can easily loosen.
“A lot of times, it doesn’t go all the way to the stomach [after swallowing],” Martin said of button batteries. “It gets stuck in the esophagus or occasionally the airway, and then in that position, it starts to create burns in those tissues and a lot of tissue damage in that area.”
That tissue damage in the esophagus and chest, Martin said, puts children particularly at risk of developing “blood vessel injuries [and] airway issues.”
“These can be very dangerous and this can absolutely be fatal,” Martin added.
“You can administer small sips of honey every couple of minutes on the way to the emergency department,” Martin explained. “It can decrease the risk of burns and tissue damage, and it can actually be lifesaving.” Martin stated.
Once gifts are open:
Immediately discard plastic wrapping or other toy packaging before the wrapping and packaging become dangerous play things.
Keep toys appropriate for older children away from younger siblings.
Battery charging should be supervised by adults. Chargers and adapters can pose thermal burn hazards to young children. Pay attention to instructions and warnings on battery chargers. Some chargers lack any mechanism to prevent overcharging.
Toy Safety Guides
The CPSC provides free safety alerts, guides, posters, brochures, handbooks and other materials which you can use to help spread consumer product safety information in your community.
During December, participate in Safe Toys and Gifts Month. Since December is the biggest gift-giving month in the world, it’s important to keep safety in mind as you’re shopping for the little ones in your life.
According to the U.S. Consumer Product Safety Commission, 251,700 toy-related injuries were treated by hospital emergency rooms around the U.S. in 2010. Of those, 72% of them were people younger than 15 years old. A few years earlier, toy makers recalled over 19 million toys across the globe due to safety concerns like lead paint and small magnets. Since then, toy safety has improved, but shoppers can take precautions to keep children in their lives safe.
Buying toys and other gifts are one of the most exciting parts about the holiday season. Who doesn’t love watching a friend or family member open a gift and seeing their eyes light up with excitement?! In all the eagerness, it’s easy to forget about simple safety. So before making any purchases this year, keep safety in mind, so the holidays don’t turn from the happiest time of the year to the scariest!
When it comes to toys and gifts, it is critical to remember to consider the safety and age range of the toys.
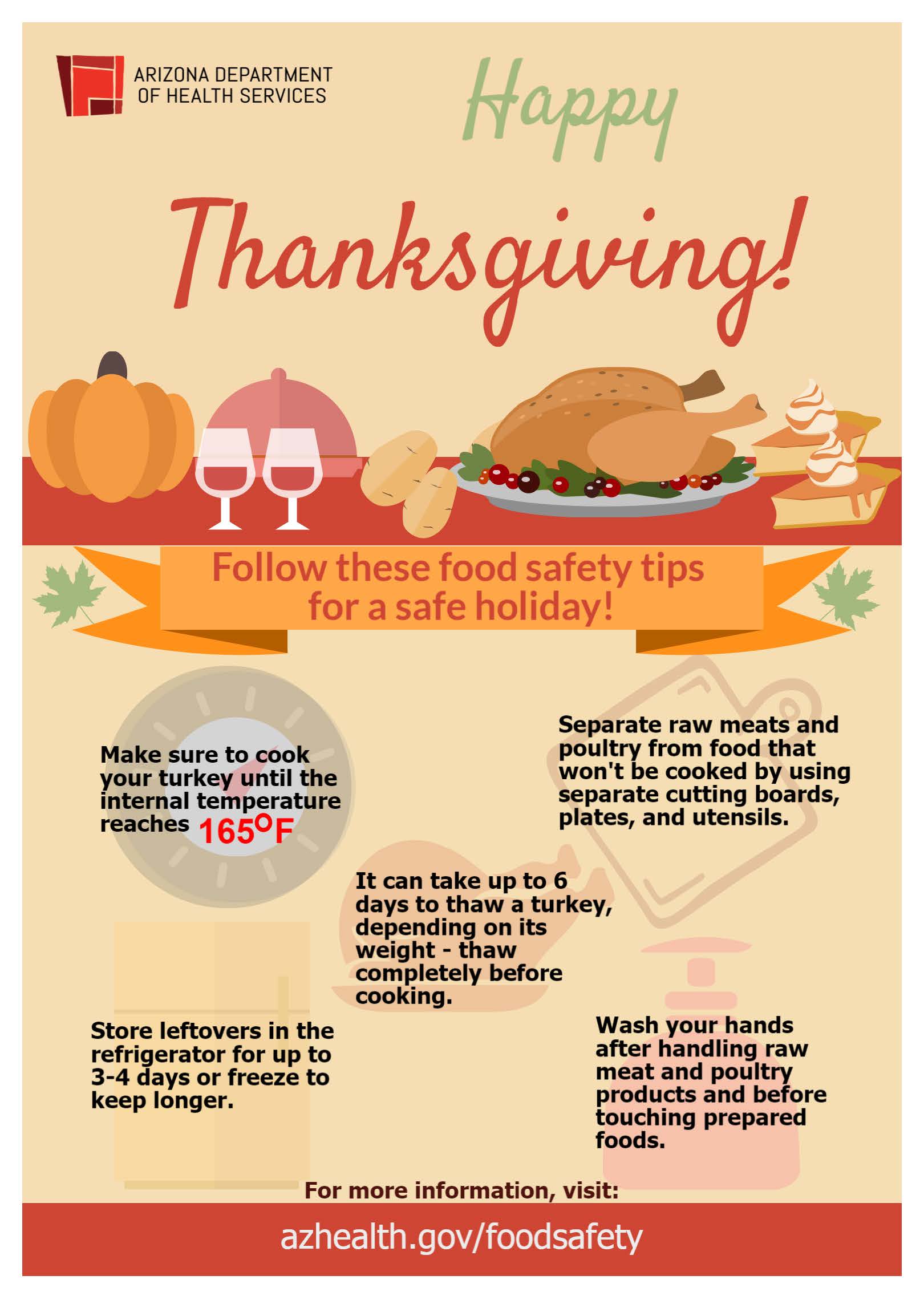
“Here’s what Martin Bucknavage, a food safety specialist at the Penn State Department of Food Science, had to say on the subject-Post holiday turkey:
“The post turkey stays good in the fridge for three to four days as a safe window if covered and refrigerated at a proper temperature. “If one is going to want to keep it longer, then it is worth considering freezing,” he says.
“Freezing is a great way to hold turkey for longer periods of time.” It’s important that if you do freeze turkey leftovers, they’re stored in a container that’s as airtight as possible.
When it comes to defrosting, it’s best to defrost in the refrigerator. However, Bucknavage explains, leftover turkey can be defrosted “under cool running water if in a hurry or thawed in the microwave, provided that it is served immediately.”
The NY post 2018 states, “The fascinating new statistic emerged in a new survey of 2,000 Americans around all things concerning Thanksgiving, which also crowned ham (60 percent), chicken (41 percent) and roast beef (37 percent) as the most popular alternatives to turkey.
The new study, conducted by Omaha Steaks, also revealed nearly half (44 percent) of Thanksgiving hosts will be serving a new main dish this year.
Thanksgiving is a delicate occasion that expects near perfection all across the board or else you risk ending up with hungry and unhappy guests.
Unfortunately, according to the study, the average Thanksgiving dinner only goes 64 percent as planned.
So what usually goes wrong? The biggest “Thanksgiving fail” is not having all the food cooked on time — with 41 percent of Americans saying they’ve been left hungry and waiting at dinner.”
Well check out about White Meat vs. Red Meat
White Meat
White meat is best known as meat that is lean, especially in comparison with red meat. The big point about white meat is that its fat content is less in comparison with red meat. Meats traditionally thought of as white (such as veal and even lamb) have been reclassified as red meats. Another advantage to eating white meat over red meat, which is also why health experts recommend it over red meat, is the lower number of calories that it contains. However, the difference in calories between white meat and red meat is not so great that it will absolutely ruin your waistline if you choose to eat some red meat once in a while.
Red Meat
Red meat is the victim of stereotypes that have been exaggerated to the point where it is today somewhat stigmatized as a food that is linked to cancer and higher fat and caloric content. While the cancer issue depends on what studies you look at and the higher caloric content is not that much over white meat, red meat does have benefits that white meat simply lacks. For example, the nutrients zinc, iron, thiamine and riboflavin (in addition to vitamins B12 and B6) appear in much greater abundance in red meat. Moreover, red meat is a great source of muscle-building protein as well as being the best source of the antioxidant called alpha lipoic acid. Still, red meat has been the subject of a lot of studies that connect it to health problems beyond cancer, like cardiovascular disease and even arthritis and hypertension.
Which One to Choose
The bottom line is that no matter which meat you eat, you can guard yourself against health problems if you eat in moderation. While white meat is not tied to as many health problems as red meat is, it does not feature many of the benefits that you get in red meat, such as the vitamins and minerals. So if you want to get a dose of said nutrients, you should eat more red meat, but do so in a way that is only moderate
HERE IS SOME FACTS ABOUT TURKEY
Because most cuts of turkey provide valuable amounts of protein, turkey is often regarded as a high-protein food. Skinned turkey breast will provide the most protein per serving, at 34 grams in 4 ounces. But you will still get 31 grams from 4 ounces of turkey leg and 21 grams from 4 ounces of turkey thigh.
In addition to protein, however, turkey is also rich in other nutrients. All B vitamins are present in turkey meat, including B1, B2, B3, B5, B6, B12, folate, biotin, and choline. (Because the biotin content of turkey meat is sensitive to the turkey’s dietary intake, the amount of this vitamin can vary greatly, with an approximate average of 0.8 micrograms in 4 ounces of turkey breast.) Turkey is a very good source for vitamin B3 and provides about 8.5 milligram in 4 ounces, or over 40% of the Daily Value (DV). It’s also a very good source of vitamin B6, at 0.64 milligrams in 4 ounces (32% DV). By providing 22%DV for choline in 4 ounces, turkey also ranks as a good source of this B vitamin.
In terms of minerals, turkey is richest in selenium and provides over 50% of the DV in a single 4-ounce serving. Zinc, copper, phosphorus, magnesium, potassium, and iron are also provided by this food in amounts varying from 5-15% DV.
All cuts of turkey contain omega-3 fats. However, the content of omega-3s in turkey can vary widely, depending on the turkey’s diet. One of the reasons we recommend pasture-raised turkey is the ability of turkeys to enjoy omega-3 containing plants and insects in natural pasture settings. As a general rule, the most favorable ratio of omega-6 to omega-3 fats is found in skinned turkey breast, where the ratio in non-pasture-raised turkey is approximately 10:1. This same ratio is about 13:1 in non-pasture-raised turkey leg or turkey thigh with skin. While there are only a few studies documenting the omega-6 to omega-3 ratio in pasture-raised turkey, those studies suggest that pasture feeding can lower the ratio to approximately 7:1. (There are some studies on pasture-raised chickens that show similar results.) Within the omega-3 family of fats, it is possible to get 10-60 milligrams of DHA (docosahexaenoic acid) from a 4-ounce serving of turkey, depending on the cut and diet consumed by the turkey. DHA is a unique omega-3 fat in terms of its ability to support healthy nerve function.
Protein Richness
When we rank all of our 100+ WHFoods based on their protein richness (how much protein they provide in comparison with their calorie content), turkey ranks first among all of our foods. A 4-ounce serving of skinned baked turkey breast provides about 34 grams of protein and over two-thirds of the Daily Value (DV). With 4 ounces of turkey leg, this number drops just slightly to 31-32 grams of protein. With 4 ounces of turkey thigh, it drops to about 21 grams. In these examples, the protein values are changing from cut-to-cut partly because of the way the turkey moves and uses its muscles, and partly because of the fat content of the various cuts. If the health benefit you are seeking from turkey is focused on protein richness, you’ll probably want to stick with skinned turkey breast as your preferred cut.
Other Health Benefits
Unfortunately, there is not as much research on turkey as there is on chicken, its fellow bird in the poultry category. Several preliminary studies show the protein richness of turkey to be of potential benefit in regulating blood sugar levels as well as insulin metabolism. These findings make sense since adequate protein intake in a balanced way throughout the day can be very helpful in managing blood sugar. In the area of cancer prevention, turkey shows that intake of it is not associated with increased cancer risk in the same way as red meats. However,they simply show that turkey intake does not raise this risk which is still a plus compared to some other foods.
Description
Like chicken, turkey belongs to the bird (Aves) class of animals, and to the family of birds called Phasianidae. While there are many different breeds of turkeys, most of them belong to the same genus and species of bird, namely Meleagris gallopavo. Turkeys are truly native to North and South America – they were not brought to the “New World” by European settlers but were instead discovered to be already present and intimately involved with Native American cultures. Turkeys are relatively large birds that can reach about 30-35 pounds in weight. They can fly short distances at speeds of about 50-55 miles per hour and run at approximately 20-25 miles per hour.
History
At 2.5 million tons of turkey meat per year, the U.S. is by far the world’s largest producer of turkey. (All countries in the European Union combined produce 1.75 million tons.) Smaller amounts of turkey are produced in Africa, Asia, and the Mediterranean. At about 450,000 tons, Brazil is the largest turkey producer in South America.
In the U.S., we consume an average of 16.5 pounds of turkey per person per year. That about is about one-quarter of our chicken consumption.
According to the National Turkey Federation, about 20% of all turkey (just over three pounds per person) is consumed on Thanksgiving Day, Gobble Gobble Day.
How to Select and Store
It’s worth taking special care in the selection of turkey! Several aspects of turkey selection will help you maximize your health benefits from this World’s Healthiest Food. First, we recommend the purchase of fresh turkey. Technically, the U.S. Department of Agriculture (USDA) guidelines allow use of the word “fresh” only when turkey has never been stored a temperature below 26°F (-3°C). (Otherwise, the term “frozen” or “previously frozen” would be required.) Additives like sodium erythorbate, MSG, and salt are not allowed on fresh turkey, and that’s a major health advantage for you.
“After a period of indulgence, your body may feel sluggish and bloated. This is often due to the consumption of high-calorie, high-sugar, and high-fat foods. Detoxing can help eliminate toxins, improve digestion, and boost energy levels. The need for detoxification arises from the accumulation of substances that can hinder your body’s natural processes. These substances can include not only the foods we eat but also environmental toxins, stress, and lack of sleep. By understanding the importance of detoxing, you can take proactive steps to support your body in its natural healing processes.
1-Staying hydrated is crucial for detoxification. Water helps flush out toxins and supports kidney function. Aim to drink at least eight glasses of water a day, and consider adding a slice of lemon for an extra detox boost.
2-Focus on consuming whole, nutrient-dense foods that support detoxification. Leafy greens, cruciferous vegetables, and fruits high in antioxidants are excellent choices. Foods such as kale, spinach, broccoli, and Brussels sprouts are packed with vitamins, minerals, and fiber, making them ideal for a detox diet. These foods help to support liver function and promote the elimination of toxins from the body. Foods rich in fiber, such as chia seeds and flaxseeds, can aid digestion and help eliminate toxins from the body. These foods act as natural cleansers, supporting your body’s detox processes. Fiber not only helps to regulate bowel movements but also promotes a healthy gut microbiome, which is essential for overall health. Consider adding fiber-rich foods to your smoothies, salads, and snacks to enhance your detox efforts. Also, healthy fats from sources like avocados, nuts, and olive oil can also support detoxification by aiding in the absorption of fat-soluble vitamins and providing essential fatty acids that promote cellular health.
Plan your meals to include a variety of nutrient-dense foods. Focus on balance and moderation, ensuring you get a mix of proteins, healthy fats, and carbohydrates. A well-rounded meal plan can help you avoid the temptation of unhealthy options and ensure that you are providing your body with the nutrients it needs to thrive.”
How to stop the eating motion and go back a step back into healthy eating after a parting day or weekend with on top leftovers. Thanks to RN NETWORK.com they have words of wisdom to offer and here they are:
“Turkey, stuffing and pie, oh my! Thanksgiving can be a stressful time for people looking to manage their weight because it is a holiday that:
1) Primarily focuses on food
2) Signifies the start of the holiday season which is full of parties, celebrations and special family meals. And unfortunately, most of these celebrations are not serving huge platters of veggies, grilled chicken, hummus and whole wheat pita with fruit for dessert!
While an all-day eating holiday like Thanksgiving can wreak havoc on otherwise good eating habits, one non-ideal meal (or day) does not lead to pounds of weight gain. The big issue for many is how to deal with the days following Thanksgiving when we have lots of temptations to keep the celebration going on. Friday (all those leftovers) and Saturday (well I’ve already gone overboard so may as well enjoy myself) and Sunday (I’ll start fresh on Monday) and Monday (I wanted to eat better but my coworkers brought in pie/cake and leftovers!) and . . . you get the idea.
To successfully tackle Black Friday, use the following three tactics:
Have a “Leftovers” Plan: We tend to run into trouble when we open the fridge the day after Thanksgiving and see tons of tempting foods staring back at us. Creating a way to control leftovers will make sure that we can indulge on our terms, not on our refrigerator’s terms (i.e. I’ve got to eat this pie and half a turkey or it will go bad). The adage still applies, “Out of sight, out of mind, out of stomach.” So if you’re hosting Thanksgiving dinner, send your guests home with care packages containing pie and casseroles. If you didn’t then send some out to neighbors, close family, bring to work or even to church to homeless. You can figure it out.
Keep Active: Nothing like falling asleep in front of the football game on TV after Thanksgiving dinner to get our weekend started on the less active foot. A great way to help our bodies deal with extra food is to keep our metabolism high throughout the weekend. Consider a bike ride, jog or workout the day after Thanksgiving into this weekend to keep you motivated to continue exercising throughout the entire holiday season. Check out the 1 hour-tip below for another activity that will let you kill two birds (pun intended) with one stone.
Preventing “Holiday Mode”: As previously mentioned, most of the issues with Thanksgiving and the holidays are when we let our celebratory meals spill into the next day, and the day after that. Many people have the the day after Thanksgiving off of work and we often are busy focusing on other activities like holiday shopping so we just go for whatever food is around: usually leftovers or eating out. Being mindful that the food-related Thanksgiving holiday ends on Thursday if not Post day is the first crucial step to setting yourself up for success over the rest of the weekend.Have 1 Minute? Give away unwanted leftovers.Have 5 Minutes? Plan a healthy Black Friday weekend.Have 15 Minutes? Portion your leftovers.Have 60 Minutes? Work out by cleaning up.
After breakfast on this weekend, get your workout in while taking care of one of the most dreaded post-Thanksgiving activities by setting aside an hour to do some vigorous cleaning all around the house if not already done. By increasing the intensity of your cleaning (a little bit faster, more elbow grease) you will clean more and burn a few hundred calories per hour.”
Sometimes the issue is not about what the leftovers are, but more how much of them are left. Spend some time Thursday night or the night after or this weekend putting the left over thanksgiving food in portion leftovers for future balanced meals for Friday and the rest of the weekend so you do not become tempted to take extra-large helpings or only eat lots of your favorite food. Freeze some leftovers too so you can enjoy them throughout the holiday season and not feel pressured to eat them all within a few days.
Plan a healthy day of eating for this weekend by writing down what you ate, from breakfast to your after-dinner snack. This will reduce that chance that you miss a meal or become tempted to eat something that is out of your routine. If you normally eat breakfast, do not skip it on Friday. Remember some of the keys to balanced meals: lean protein, complex carbs, plenty of fruits and veggies and healthy fats (avocado, olive oil, nuts, salmon, etc.). Consistency is key: make sure you eat on Friday the same way you ate the month, week and day before Thanksgiving.
Create a leftover delegation list with each family or person coming to Thanksgiving and the associated foods you will send them home with. Ask guests to bring their containers with them or make sure you have enough that you don’t mind parting with.
About the author: Jason Machowsky, MS, RD, CSCS is a registered dietitian, certified personal trainer.
“The winter holidays can turn deadly as research shows that more people die from heart attacks that season! While being aware of the signs of a heart attack and taking steps to reduce your risk are important all year long, the American Heart Association, the world’s leading voluntary organization focused on heart and brain health for all, says that’s especially critical during the next few weeks.”
The symptoms indicating a Myocardial Infarction or Heart Attack:
Chest pain or discomfort-Pain or discomfort in the jaw, neck or back
Pain or discomfort in the arms or shoulders Shortness of breath Feeling very tired or lightheaded or faint-Remember for many which is more men asymptomatic in many cases other than possibly feeling just weak or faint. Nausea or vomiting
**If any the symptoms are present call 911!**
The sooner you get the pt to the ER the better; especially if no defibrillator is present where the person having a MI is located and if he or she needs it!! Time matters including what treatment is needed! The sooner the treatment the better in many cases regarding the ending result of the person’s condition. Since the sooner the treatment the better where in a lot of cases the ending result for the pt having an MI is worse due to prolonging medical treatment. An MI is scarring of the heart tissue where the MI occurred due to lack of oxygen to that area of the heart and is not reversible! The sooner the treatment the less damage to the heart in many cases with better results!
It’s the holiday season—cardiac patients not careful in eating but indulging in junk food may put you at high risk for a bomb to go off in the heart=heart attack.
While colder weather may play a role, studies have shown that the spike in heart events during the holiday season occurs even in It’s no secret that holiday celebrations offer many temptations to overindulge. Many holiday foods are high in saturated fats or sodium. Overindulgence in these foods can increase cholesterol levels or blood pressure, making it more difficult for blood to flow through arteries and upping the chance of a blockage. What you may not know is that eating a heavy holiday meal may affect you even after you’ve pushed away from the table. “Research shows that anyone with coronary-artery disease or high cholesterol has a heightened risk for heart attack for up to one day after eating a heavy meal,” said Mittleman. Mittleman participated in a study, “Heavy Meals May Trigger Heart Attacks,” led by Francisco Lopez-Jimenez, MD, currently the Director of the Cardio-metabolic Program at the Mayo Clinic. This study, which focused on nearly 2,000 former heart attack patients, found that 10 percent of them suffered a coronary within 26 hours of eating a heavy meal.
“People often change their eating habits during the holidays,” said Dr. Anne Riley, a cardiologist at BIDMC. “For those with congestive heart failure [CHF], salty foods can cause fluid retention and high blood pressure, which place added stress on an already weakened heart.”
Your heart may leap with delight on the couch after Thanksgiving or at the electronic gizmo or emerald bracelet that you’ve just unwrapped from under the Christmas tree. But you can’t say the same for that nasty holiday surprise known as the “Happy Thanksgining” or “Merry Christmas coronary” or “Happy Hanukkah heart attack.”
For many years, researchers have been intrigued by a disturbing pattern: Deadly heart attacks increase during the winter holiday season. One study even found distinct spikes around Christmas and New Year’s Day.
Recommended Related to Heart Health
Read Amazing Facts About Heart Health and Heart Disease:
You can feel your heart thudding away every time you put your hand to your chest, but do you have any idea what’s really going on in there or what keeps your heart ticking as it should? WebMD the Magazine asked Richard Krasuski, MD, director of Adult Congenital Heart Disease Services and a staff cardiologist at the Cleveland Clinic, to help explain some amazing and little-known facts about the human heart.
“We certainly know that there are certain risk factors for coronary artery disease. There’s obviously smoking, hypertension, dyslipidemia [high cholesterol], diabetes, lack of exercise, and age,” says Robert A. Kloner, MD, PhD, a researcher at Good Samaritan Hospital in Los Angeles and a professor at the Keck School of Medicine at the University of Southern California.
“But we’re also learning that there are certain triggers for cardiovascular events,” he adds, “including time of the year and seasons. If we can get a true handle on the seasonal variation, we could knock down death from coronary disease.”
Coronary artery disease stems from atherosclerosis, a condition in which fatty plaques narrow the arteries to the heart. When a plaque ruptures, it can trigger a blood clot that leads to a heart attack.
In a national 2004 study published in Circulation, researchers at the University of California, San Diego, and Tufts University School of Medicine examined 53 million U.S. death certificates from 1973 to 2001. They discovered an overall increase of 5% more heart-related deaths during the holiday season. When researchers looked at individual years, they found varying increases in cardiac deaths for every holiday period they studied, except two.
Doctors have long known that cold weather is hard on the heart. Blood vessels constrict, which raises blood pressure. Blood also clots more readily. Frigid temperatures increase strain on the heart, and too much physical exertion can worsen the burden and trigger a heart attack. For example, doctors have treated many patients whose heart attacks followed strenuous snow shoveling.
Not to put a damper on holiday frivolity, but heart attacks increase during winter. For one reason, cold weather is tough on the heart. Blood vessels constrict, which causes blood pressure to rise. Additionally, blood clots more easily. (I’m getting this info, by the way, from the boldface link a sentence or two ago).
“People tend to consume much more fat, salt, sugar, and alcohol during the holiday season,”. “Also, people tend to be less active due to the cooler weather. Overindulgence of food and alcohol along with inactivity raises the blood pressure and cholesterol levels. These risk factors combined increase your chances of having congestive heart failure, a stroke, or even a heart attack.” says Roberto Wayhs, MD, chief of cardiology at Methodist Charlton Medical Center.
To put a stop to that, or at least decrease your chances, he offers these tips:
Limit foods and beverages that are salty and/or rich. Blood pressure tends to go up the more salt you intake. Rich and sugary foods raise blood sugar levels.
Be consistent in taking your daily medications. You need them at all times of the year to maintain good health.
Get enough sleep. Sleep loss is related to weight gain, which also can affect the heart. Aim for at least seven hours.
Control your stress. “Holiday sadness adds stress,” Wayhs says. “Don’t be afraid to seek professional help if you need it.”
Limit alcohol intake. “High alcohol intake has been linked to irregular and rapid heartbeats (atrial fibrillation) and congestive heart failure,” says Dr. Wayhs.
Maintain your normal exercise routine. “Don’t place your healthy habits on the back burner,” he says.
If you don’t have time for your usual workouts, try a shorter one.
Oh and, of course, stop smoking. But you knew that already.
“Thanksgiving for many people is a time to just cook and eat. I’m sure for most, there’s a lot of nostalgia around the dishes on the table. I also know that for many people on health and wellness journeys, this time of year can bring up anxiety around food. Here are some Thanksgiving healthy eating tips to share so that you can still indulge with your loved ones this holiday season, while also balancing your plate with nourishing, nutrient-dense foods, all without feeling like you’re missing out on your favorite dishes.
Have you ever heard the saying “eat the rainbow”? Adding color and variety to your plate doesn’t only make your tablescape look incredible—it also helps ensure that you’re getting a variety of essential nutrients in your meal. Vegetables are the perfect vessel to add vibrant color and rich flavor to any meal. Vegetables are also an excellent source of fiber, helping us feel full and satisfied. Vegetables can also balance heavier, starchier sides with bright, fresh flavors, crunchy texture, and vivid color.
Fill half your plate with veggies. Loading up on colorful, non-starchy vegetables first will increase fiber intake and promote fullness, and help to manage portions of the higher-calorie dishes.
Opt for whole grains if available. These foods will provide more fiber and nutrients compared to refined or white grains, avoiding a blood-sugar spike and helping you feel fuller longer.
Hydrate wisely. Drink water before and during the meal to help you feel full and decrease mindless eating.
Be mindful of high-calorie additions. Toppings like butter, gravy and cream-based sauces can add a lot of calories and saturated fats. Consider lighter alternatives or using smaller portions.
Have fun and enjoy the company of those around you.”
Eating slowly, putting your fork down between bites, and tasting each mouthful is one of the easiest ways to enjoy your meal and feel satisfied with one plate full of food, experts say. Choosing whole grains, fruits, vegetables, broth-based soups, salads, and other foods with lots of water and fiber add to the feeling of fullness.
Spread out the food and fun all day long. At the Finn family Thanksgiving gathering, they schedule dessert after a walk, while watching a movie together.
“We eat midday, and instead of another meal at dinnertime, we continue the feast with dessert a few hours after the main meal,” Finn explains.
Go Easy on Alcohol
Don’t forget those alcohol calories that can add up quickly.
“Have a glass of wine or a wine spritzer and between alcoholic drinks, (or) enjoy sparkling water,” says Diekman. “this way you stay hydrated, limit alcohol calories, and stay sober.”
Be Realistic
The holiday season is a time for celebration. With busy schedules and so many extra temptations, this is a good time to strive for weight maintenance instead of weight loss.
“Shift from a mindset of weight loss to weight maintenance,” says Finn. “You will be ahead of the game if you can avoid gaining any weight over the holidays.”
Everyone looks forward to Thanksgiving for the delicious food (and, of course, the leftovers!). But did you know that the average adult eats approximately 2000-3000 calories at the Thanksgiving meal? Try the following strategies so you still can enjoy your meal more while making it more healthful (and less caloric):
Don’t come to the Thanksgiving table starving! Make sure to have a healthful breakfast and lunch before arriving at dinner. When you are extremely hungry, you eat very fast and tend to overeat.
Fill your plate with salad and veggies first and then leave a small amount of space for higher calorie options like stuffing, mashed potatoes, green bean casserole, etcetera. Don’t deprive yourself of your favorite dishes—think in terms of moderation!
Distance yourself from the hors d’oeuvre table. Munch on fresh fruits and vegetables (preferably organic) instead of high fat appetizers.
Drink plenty of water to keep your body hydrated, many of the foods served on Thanksgiving are high in sodium.
Go skinless…most of the fat is in the turkey skin. Have your turkey breast, leg, or thigh without the skin to trim major calories and fat. (Have you ever thought of trying a vegetarian Thanksgiving? It’s a radical concept for many, but it’s a fun way to think creatively in the kitchen about the holiday.)
Eat slowly…put your fork down every few bites and drink water. Your brain will have time to catch up with your stomach and you will find that you are satisfied with less food!
If you are the host, try making healthful alternatives such as steamed green beans with a drizzle of olive oil and almond slivers (instead of green bean casserole) and baked sweet potatoes (instead of baked yams with butter and marshmallows) to decrease calories and fat and increase nutrient density!