
The N.Y. State Health Department states the following:
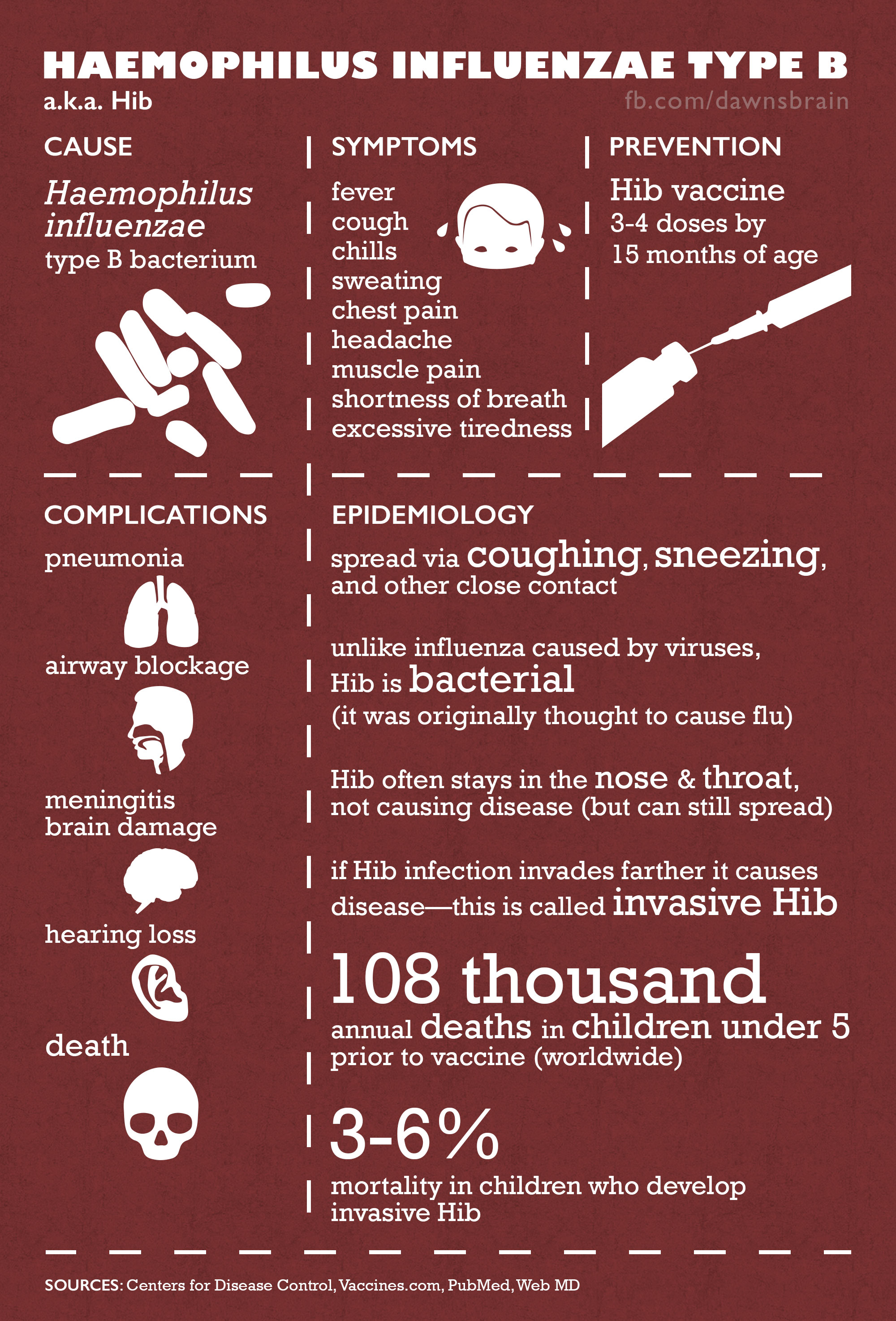
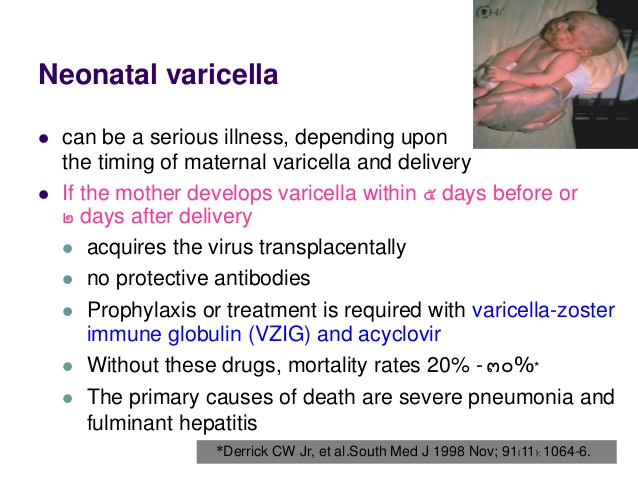
There are many reasons parents give for delaying a vaccination, from “My baby cries when she gets the shot,” to “My child is too young to get so many vaccines.” More important than all of these excuses is one simple fact: A child’s immune system is more vulnerable without vaccinations. And if it weren’t for vaccinations, many children could become seriously ill or even die from diseases such as measles, mumps and whooping cough.
We live in an increasingly global world, with increased risks around every corner. Travelers entering into New York create an even greater risk of exposure. On a regular basis there is a new report regarding a disease outbreak somewhere in the world – including in the United States and New York State. The Centers for Disease Control and Prevention reports outbreaks around the world and provides health information for travel to more than 200 international destinations. (cdc.gov) From mumps, to pertussis to the measles, diseases once thought to be eradicated are coming back because people are not being vaccinated as they once were. If you think tears from a needle are hard to watch, imagine the suffering your child will experience if he or she contracts a serious disease that could have been prevented.
While misinformation in the media has led many parents to delay vaccinations as a result of either Dr. Andrew Wakefield’s false claims about autism or Dr. Bob’s Alternative Schedule (aap.org), many diseases have begun to reemerge among children around the world. Don’t let your child become a statistic — make sure they get all the recommended vaccinations. And if you’re worried about autism, visit “The Truth About Autism.”
Yes there are side effects to vaccinations but the odds are slim and the reason for the vaccinations in childhood including adulthood outweighs the possible risk for side effects. I have been a RN 31 years and have received the MMR (measles, mumps, and rubella) every 10 years, flu every year, & pneumonia every 5 years and have never gotten a side effect from them.
The threat of death by disease isn’t the only medical consequence of skipping vaccinations. An unvaccinated child faces lifelong differences that could potentially put him or her at risk. Every time you call 911, ride in an ambulance, go to the doctor or visit the hospital emergency room, you must alert medical personnel of your child’s vaccination status so he or she receives distinctive treatment. Because unvaccinated children can require treatment that is out of the ordinary, medical staff may be less familiar, and less experienced, with the procedures required to appropriately treat your child.
Women who are pregnant but not vaccinated can be vulnerable to diseases that may complicate their pregnancy. A pregnant woman who contracts rubella in the first trimester may have a baby with congenital rubella syndrome (CRS), which can cause heart defects, developmental delays and deafness.
People who choose not to vaccinate their children also put others at risk if their child isn’t vaccinated and becomes ill. Special groups of people cannot be vaccinated, including those with compromised immune systems (e.g. those with leukemia or other cancers). These people rely on the general public being vaccinated so their risk of exposure is reduced.
There are also social implications of not vaccinating your child — from exclusion to quarantine. If sick or exposed to disease, your child may need to be isolated from others, including family. If there is an outbreak in your community, you may be asked to take your child out of school and other organized activities, causing your child to miss school and special events. Your child’s illness or inability to go about their daily activities also may impact your work and household income. For more information on vaccination requirements for schools in the state of New York, see New York State Immunization Requirements for School Entrance/Attendance (PDF, 71KB, 2pg.).
Everyone 6 months and older should get a seasonal flu vaccine every year. It’s important to reiterate that every year the flu remains a threat, and every year children still die as a result of having the flu. One of those children was Joseph Marotta. At 5 years old, Joseph contracted the flu. Less than 10 days after contracting the flu, Joseph died. His parents, along with other members of Families Fighting Flu (familiesfightingflu.org), are strong advocates for annual flu vaccines and encourage all families to get vaccinated. It’s important that everyone 6 months and older receives an annual flu vaccine. Every year a flu vaccine is skipped, your child is at risk.
The CDC states:

 Temporary Solution
Temporary Solution