Statistics to know about strokes:
Stroke was the third leading cause of death in the United States. Presently the CDC says under its statistics that Stroke is the fifth leading cause of death for Americans, but the risk of having a stroke varies with many factors. Remember strokes have declined since 2003 based on CDC risk factors now compared to risk factors CDC listed in 2014.
More than 140,000 people die each year from stroke in the United States, that’s 1 out of every 20 deaths now.
Stroke costs the United States an estimated $34 billion each year. This total includes the cost of health care services, medicines to treat stroke, and missed days of work.
Stroke is the leading cause of serious, long-term disability in the United States. Each year, approximately 795,000 people suffer a stroke.
About 600,000 of these are first attacks, and 185,000 are recurrent attacks. Nearly three-quarters of all strokes occur in people over the age of 65. Stroke reduces mobility in more than half of stroke survivors age 65 and over.
The risk of having a stroke more than doubles each decade after the age of 55.
Strokes can & do occur at ANY age. Nearly one fourth of strokes occur in people under the age of 65. Stroke risk increases with age, but strokes can—and do—occur at any age.
In 2009, 34% of people hospitalized for stroke were less than 65 years old.
Stroke death rates are higher for African-Americans than for whites, even at younger ages.
On average, someone in the United States has a stroke every 40 seconds.
Stroke accounted for about one of every 17 deaths in the United States in 2006. Stroke mortality for 2005 was 137,000.
From 1995–2005, the stroke death rate fell ~30 percent and the actual number of stroke deaths declined ~14 percent. It still has declined from 2005 by CDC statistics which is good.
While stroke death rates have declined for decades among all race/ethnicities, Hispanics have seen an increase in death rates since 2013.
What is a Stroke?
A Stroke is a disease that affects the arteries leading to and within the brain. It is the No. 5 cause of death and a leading cause of disability in the United States. A stroke occurs when a blood vessel which carry oxygen and nutrients to the brain is either blocked by a clot or bursts (or ruptures). When that happens, part of the brain cannot get the blood (and oxygen) it needs, so this in the end causes brain cells to die.
There is a stroke noted as a mini stroke which is a transient (temporary) ischemic attack= TIA, which we went over last Friday. If you want to review it go right ahead, its listed under 5/08/2020 article. A TIA is different than strokes. First some call it a mini stroke but remember the symptoms of a TIA are similar to stroke symptoms listed below for actual strokes; the difference for the patient is that they are completely reversible. Take angina for example, in this case the pt has the heart affected but the symptoms are completely reversible, just a different organ. The organs (the heart for angina and the brain for TIA) are simply having the symptoms of an infarction of the organ that is involved but both are due to lack of 0xygen, called ischemia.
Getting back to actual strokes lets review types of strokes.
There are 2 types of strokes:
Ischemic Stroke which are strokes that occur through an obstruction of blood flow by a clot called a thrombus.
Hemorrhagic stroke by a blood vessel rupturing and preventing blood flow to the brain.
In the case of a stroke its a infarction to the brain due to lack of oxygen to the organ we call the brain, only the symptoms are not reversible but they can decrease in the intensity of the damage the caused in time with treatment (PT and OT) in time. For some the symptoms are almost completely gone, again it depends on the intensity of the stroke to the brain, how bad was it with the symptoms it caused.
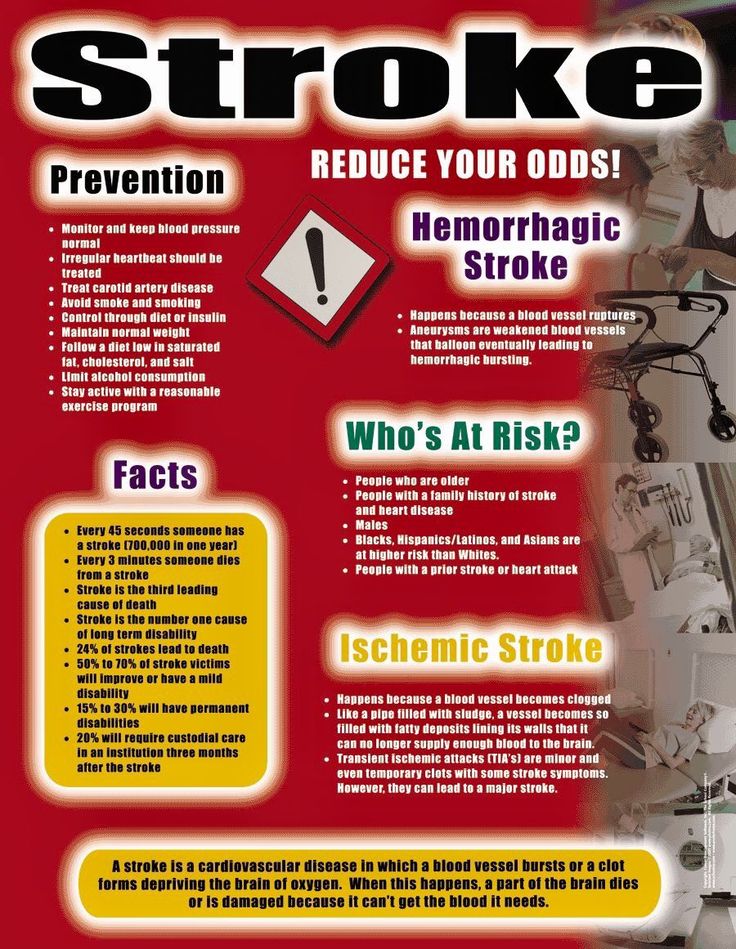
What are the risk factors for a stroke?
Non modiafiable risks meaning you can’t change them are:
–Age: Stroke occurs in all age groups. Studies show the risk of stroke doubles for each decade between the ages of 55 and 85. But strokes also can occur in childhood or adolescence. Although stroke is often considered a disease of aging, the risk of stroke in childhood is actually highest during the perinatal period, which encompasses the last few months of fetal life and the first few weeks after birth.
-Gender: Men have a higher risk for stroke, but more women die from stroke. Men generally do not live as long as women, so men are usually younger when they have their strokes and therefore have a higher rate of survival.
-Race: People from certain ethnic groups have a higher risk of stroke. For African Americans, stroke is more common and more deadly—even in young and middle-aged adults—than for any ethnic or other racial group in the United States. Studies show that the age-adjusted incidence of stroke is about twice as high in African Americans and Hispanic Americans as in Caucasians. An important risk factor for African-Americans is sickle cell disease, which can cause a narrowing of arteries and disrupt blood flow. The incidence of the various stroke subtypes also varies considerably in different ethnic groups.
–Family history of stroke: Stroke seems to run in some families. Several factors may contribute to familial stroke. Members of a family might have a genetic tendency for stroke risk factors, such as an inherited predisposition for high blood pressure (hypertension) or diabetes. The influence of a common lifestyle among family members also could contribute to familial stroke.
Modiafiable Risk Factors meaning you CAN change them:
–High Blood Pressure (hypertension)
RX: DIET & EXERCISE & MEDS that a MD would decide.
–High Cholesterol
RX: DIET and if necessary MEDS that a MD would decide.
–Diabetes Mellitus
RX: DIET & EXERCISE & MEDS that a MD would decide.
–Cigarette Smoking
RX: QUIT
–Carotid Artery Disease
RX: DIET & EXERCISE & MEDS even possible SURGERY that a MD would decide.
–Atrial Fibrillation
RX: DIET & EXERCISE & MEDS even possible SURGERY that a MD would decide.
–Unhealthy Diet RX: DIET
–Physical Inactivity and Obesity
RX: DIET & EXERCISE & possibly even MEDS that a MD would decide.
Go to your DOCTOR before doing any program and let your MD tell you what type of a program would be best for you especially if you are diagnosed with disease (EX. Diabetes, Cardiac, etc…).