Affects older persons; peak incidence between 6 -7th decades. Tumor cells secrete an M protein (commonly IgM) Mixture of B cells ranging from small lymphocytes to plasmacytic lymphocytes to plasma cells. Involves lymph nodes, bone marrow, and spleen at presentation.
Initially, you will need to learn some basics about Waldenstrom’s macroglobulinemia (WM), sometimes referred to as a lymphoplasmacytic lymphoma (LPL). Newly diagnosed? Well striveforgoodhealth.com understands that this is a very difficult time for you. Not only are you, your family and your friends experiencing the gamut of different emotions that come with a cancer diagnosis, but there is so much new information to learn.
Here’s one place to start in getting information on this diagnosis!
Let’s understand first what is effected in the body and answer the questions that probably you are asking yourself (pt or family or friends).
What is effected in this disease?
B Lymphocytes are effected; they are a type of white blood cell that makes antibodies. B lymphocytes are part of the immune system and develop from stem cells in the bone marrow. Same with T cells. T- and B-cells are highly specialized defender cells – different groups of cells are tailored to different germs. When your body is infected with a particular germ, only the T- and B-cells that recognise it will respond. These selected cells then quickly multiply, creating an army of identical cells to fight the infection. Special types of T- and B-cells ‘remember’ the invader, making you immune to a second attack.
What’s so special about the B cells?
With the help of T-cells, B-cells make special Y-shaped proteins called antibodies. Antibodies stick to antigens on the surface of germs, stopping them in their tracks, creating clumps that alert your body to the presence of intruders. Your body then starts to make toxic substances to fight them. Patrolling defender cells called phagocytes engulf and destroy antibody-covered intruders.
With this disease what happens to the B Cells?
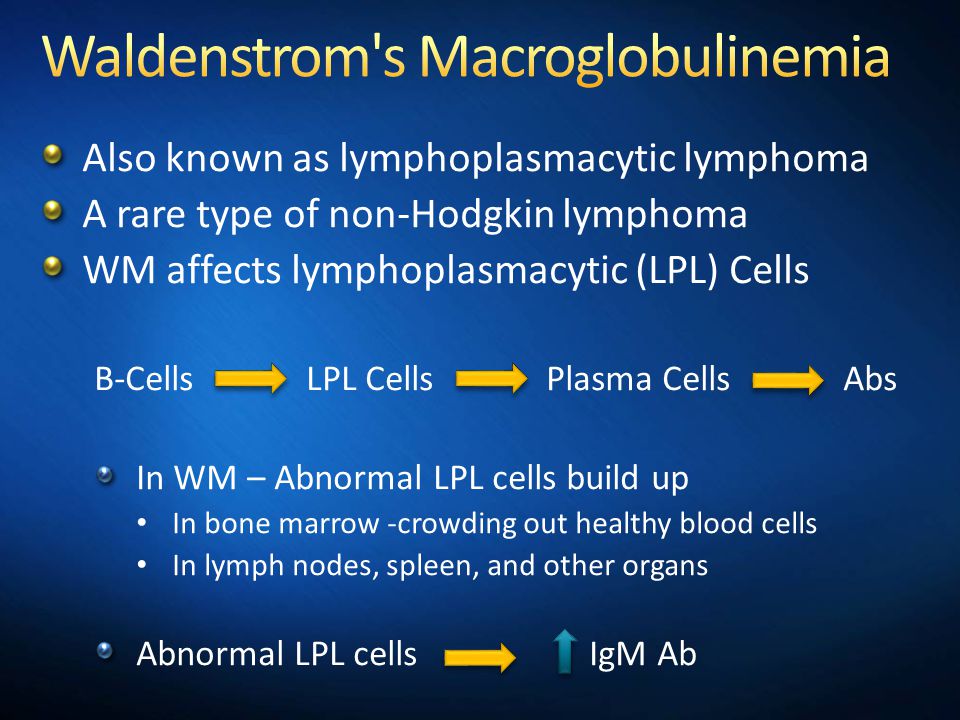
When diagnosed with Waldenstrom’s macroglobulinemia (WM) which is a lymphoma or cancer. It affects a type of white blood cell called a B-lymphocyte or B-cell, which normally matures into a plasma cell whose job is to manufacture immunoglobulins (antibodies) to help the body fight infection. In WM, there is a malignant change to the B-cell in the late stages of maturing and it continues to proliferate as a clone of identical cells, primarily in the bone marrow, but also in the lymph nodes and other tissues and organs. It is known as lymphoplasmacytic lymphoma (LPL) and must be associated with the production of an antibody protein or immunoglobulin known as IgM in order for WM to be diagnosed.
What’s the difference of WM versus LPL? Are they the same disease?
Sometimes WM and LPL (lymphoplasmacytic lymphoma) are used interchangeably although WM is really an LPL. However, WM comprises about 90 – 95% of all LPL patients.
The median survival has varied in studies, from 5 years to 10